Obesity Pathophysiology — Hormonal, Metabolic & Neural Drivers
Clinical Use Only — Licensed Prescriber Education
This content is for educational use by licensed medical prescribers (MD, DO, NP, PA) and pharmacists operating within their scope of practice. It is not intended for use by patients or non-licensed individuals.
Peptides and small molecules discussed include drugs approved for marketing claims for one or more named indications, drugs in active Phase 3 development, drugs with regulatory submission pending, and substances available through 503A/503B compounding pharmacy pathways. Regulatory status varies by US state and country; clinicians remain responsible for verifying the legal status of any compound in their jurisdiction of practice before prescribing, administering, or dispensing.
"Approved for marketing claims" — a clarified nuance. When we say a drug is "approved," we mean the regulator has granted marketing claims for one or more named indications based on adequate evidence of safety and efficacy. Approval is indication-specific, not drug-level: a molecule approved for type 2 diabetes and chronic weight management is approved-for-marketing-claims for those indications; using the same molecule for an indication outside the label is "off-label use of an approved drug," not "use of a non-approved drug." Throughout Module 5 we follow the convention "approved for marketing claims for [indication X]; off-label for [indication Y]" wherever both registers apply, and "pre-approval-for-marketing-claims" for compounds whose registration is pending.
Nothing in this course constitutes medical advice for any specific patient. All clinical decisions remain the responsibility of the treating provider. Synergy Health AI Academy provides research education only; it does not establish a provider-patient relationship with course participants or their patients.
Dosing, indications, and protocols reflect current published evidence and practitioner consensus. Individual patient response varies; titrate and monitor per clinical judgment.
═══════════════════════════════════════════════════════════════════════
OPENING
Obesity care has moved into a different phase of its history. Over the last five years, peer-reviewed Phase 3 evidence has accumulated across an expanding class of neuroendocrine therapeutics — single GLP-1 receptor agonists (semaglutide, liraglutide), dual GLP-1/GIP coagonists (tirzepatide), dual GLP-1/glucagon agonists (survodutide), triple GLP-1/GIP/glucagon agonists (retatrutide), amylin analogs (cagrilintide), and the first oral non-peptide GLP-1 receptor agonist (orforglipron) — with reproducible double-digit body-weight reductions across unselected adult populations. Combination products co-formulating two distinct mechanism components in a single weekly injection (CagriSema, insulin icodec + semaglutide) extend the design space further. By the time a clinician finishes residency today, the comparator landscape will have shifted at least once.
The implication for clinical practice is not memorization. It is mechanism. The clinicians who can move with the evidence are the ones who understand the underlying biology: the neuroendocrine signaling architecture, the set-point defense, the phenotypic heterogeneity of obesity itself, and the mechanism-class differentiation among the agents now in routine and near-future use. The clinicians who only know the current dosing chart will be retraining every eighteen months.
This lesson establishes that foundation. It is intentionally compact — your time is finite, and this is a foundational lesson, not a textbook. The aim is to give you the mechanistic frame that makes every subsequent lesson in Module 5 — semaglutide deep dive, tirzepatide, the GLP-1/GIP/glucagon class, the amylin axis, lean-mass preservation, titration, monitoring, lab interpretation, case construction — read as a logical sequence of interventions against a defined biology, not a catalog of memorized protocols. The work the lesson does is to make obesity legible as a chronic neuroendocrine disease with a defended set point, a multi-axis hormonal architecture, and a now-mature pharmacological vocabulary for engaging that architecture across multiple mechanism classes.
═══════════════════════════════════════════════════════════════════════
Module: M5 | Duration: 1.5h (+ FAQ appendix) | Type: Lecture
LEARNING OBJECTIVES
By the end of this lesson, the clinician will be able to:
- Describe the neuroendocrine regulation of appetite and energy balance, including the amylin axis as a non-incretin satiety pathway
- Identify the key hormonal axes engaged by current and near-future pharmacotherapy (GLP-1, GIP, glucagon, amylin, leptin, ghrelin, insulin)
- Explain metabolic adaptation and the defended set point, and articulate the clinical implications for combined pharmacotherapy + lifestyle intervention
- Map the current mechanism-class taxonomy across single GLP-1 RAs, dual coagonists, triagonists, amylin analogs, oral non-peptide platforms, and combination products
- Apply patient phenotyping to guide first-line agent selection within the mechanism-class taxonomy
- Articulate the boundary between established Phase 3 evidence, sponsor-disclosed pending publications, and active research directions
MODULE MAP
This lesson sits at the front of Module 5 because every subsequent lesson is an answer to a question this lesson raises. M5.2 covers semaglutide in depth — the dominant first-line single GLP-1 RA for appetite-driven phenotypes, anchored by the SELECT cardiovascular evidence and the STEP/SUSTAIN/FLOW programs. M5.3 covers tirzepatide — the dual GLP-1/GIP coagonist mapping onto metabolic / insulin-resistant phenotypes plus the SURMOUNT-1/-2/-5 efficacy frontier. M5.4 surveys liraglutide as the predecessor compound plus the active Phase 3 frontier (retatrutide, survodutide, orforglipron, aleniglipron, MariTide, mazdutide) so clinicians can read the literature as it lands. M5.5 turns to tesamorelin and AOD-9604 for visceral and stubborn-fat phenotypes. M5.6 addresses lean-mass preservation — central to the long-term durability of any weight intervention on the GLP-1 axis. M5.7 covers GHK-Cu protocols for post-loss skin laxity that drives discontinuation in real practice.
The back half of the module is workflow. M5.8 is titration and side-effect management — where most clinical errors happen. M5.9 is the lab-monitoring panel (HbA1c, lipids, insulin, leptin, body composition). M5.10 is an integrated case. The four clinical workflows the module is built around — phenotyping → mechanism-class agent selection → titration → monitoring — map onto 5.1 → 5.2–5.5 → 5.8 → 5.9. If you can run that loop confidently, you can practice this medicine across the current and near-future pharmacopeia.
═══════════════════════════════════════════════════════════════════════
LESSON CONTENT
Section 1: The Neuroendocrine Model of Obesity (30 min)
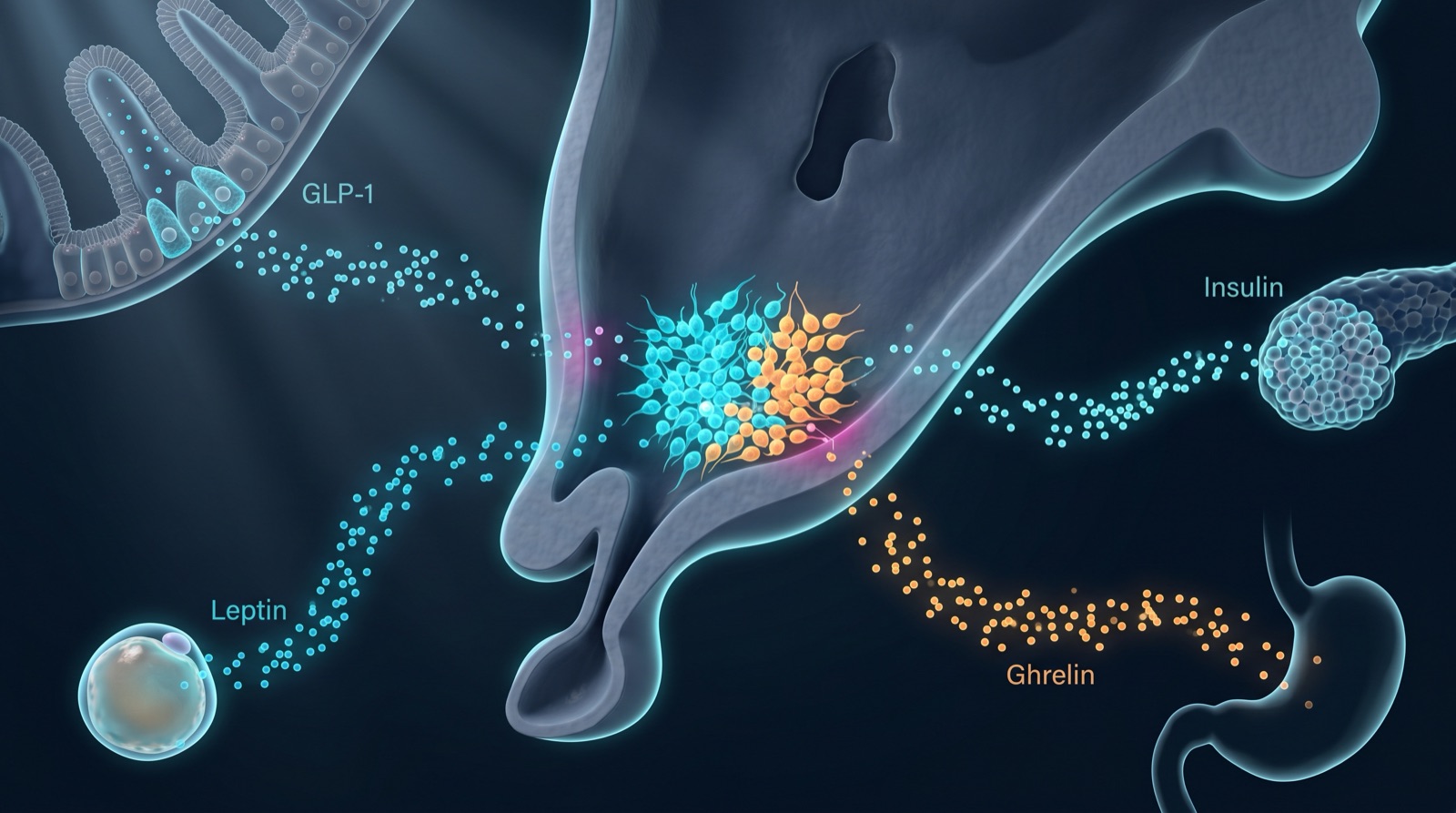
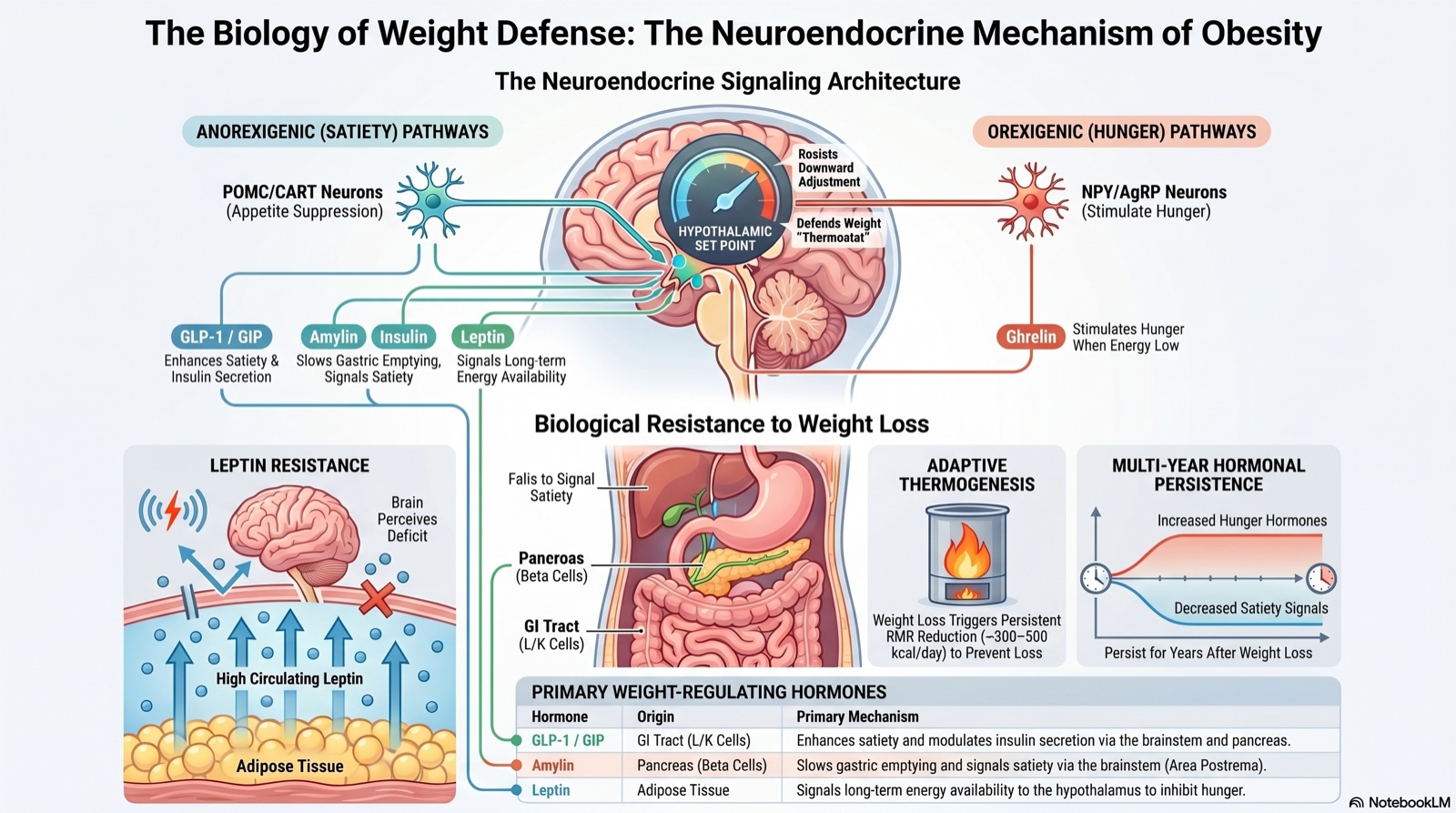
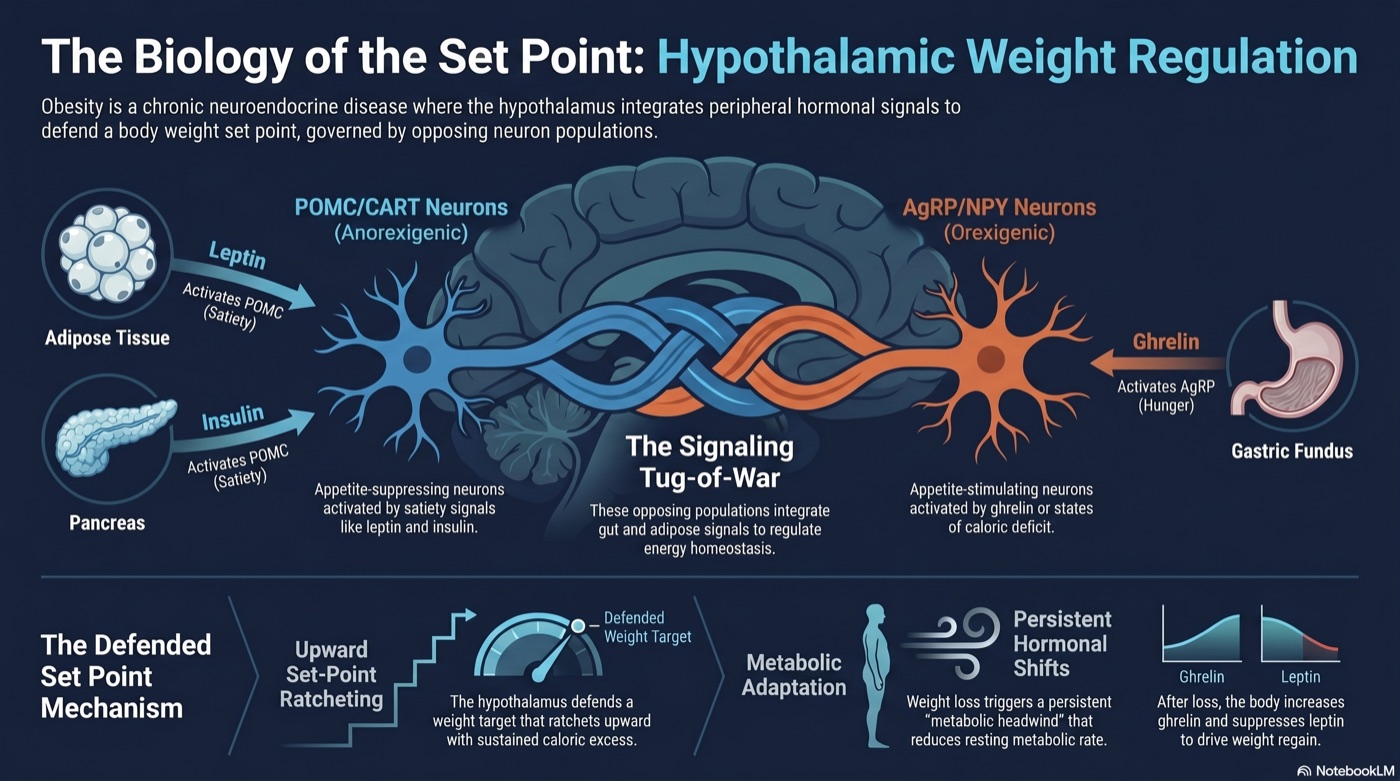
Obesity is a chronic, relapsing neuroendocrine disease. The hypothalamus integrates peripheral signals from adipose tissue (leptin), the gastrointestinal tract (GLP-1, GIP, PYY, ghrelin, CCK), the pancreas (insulin, amylin), the brainstem area postrema and nucleus tractus solitarii (which sit functionally outside the blood-brain barrier and act as the primary receiver site for circulating satiety peptides), and the liver to regulate energy homeostasis through opposing pathways.
Anorexigenic (appetite-suppressing) signals:
- Leptin (from adipocytes) → activates POMC/CART neurons in the arcuate nucleus
- GLP-1 (from L-cells of ileum/colon, and from preproglucagon neurons in the brainstem NTS) → delays gastric emptying, reduces appetite via central and vagal pathways
- GIP (from K-cells of duodenum/jejunum) → incretin effect, augments glucose-dependent insulin secretion, modulates adipose lipid handling
- PYY (from L-cells) → reduces food intake via Y2 receptors on arcuate NPY/AgRP neurons
- Amylin (co-secreted with insulin from pancreatic β-cells at a roughly 1:100 amylin:insulin molar ratio) → engages amylin receptors (CTR + RAMP1/2/3 heterodimers) at the brainstem area postrema and NTS, slows gastric emptying, suppresses postprandial glucagon
- CCK (from duodenal I-cells) → vagal afferent satiety signaling
- Insulin (in physiologic concentrations) → hypothalamic satiety signal via insulin-receptor expression on POMC neurons
Orexigenic (appetite-stimulating) signals:
- Ghrelin (from gastric fundus) → activates NPY/AgRP neurons → hunger
- Endocannabinoids → CB1 receptors in hypothalamus → appetite stimulation
- Cortisol (in chronic excess) → drives visceral fat deposition, increases appetite
- Low leptin (in caloric deficit or sustained weight loss) → removes the POMC satiety brake
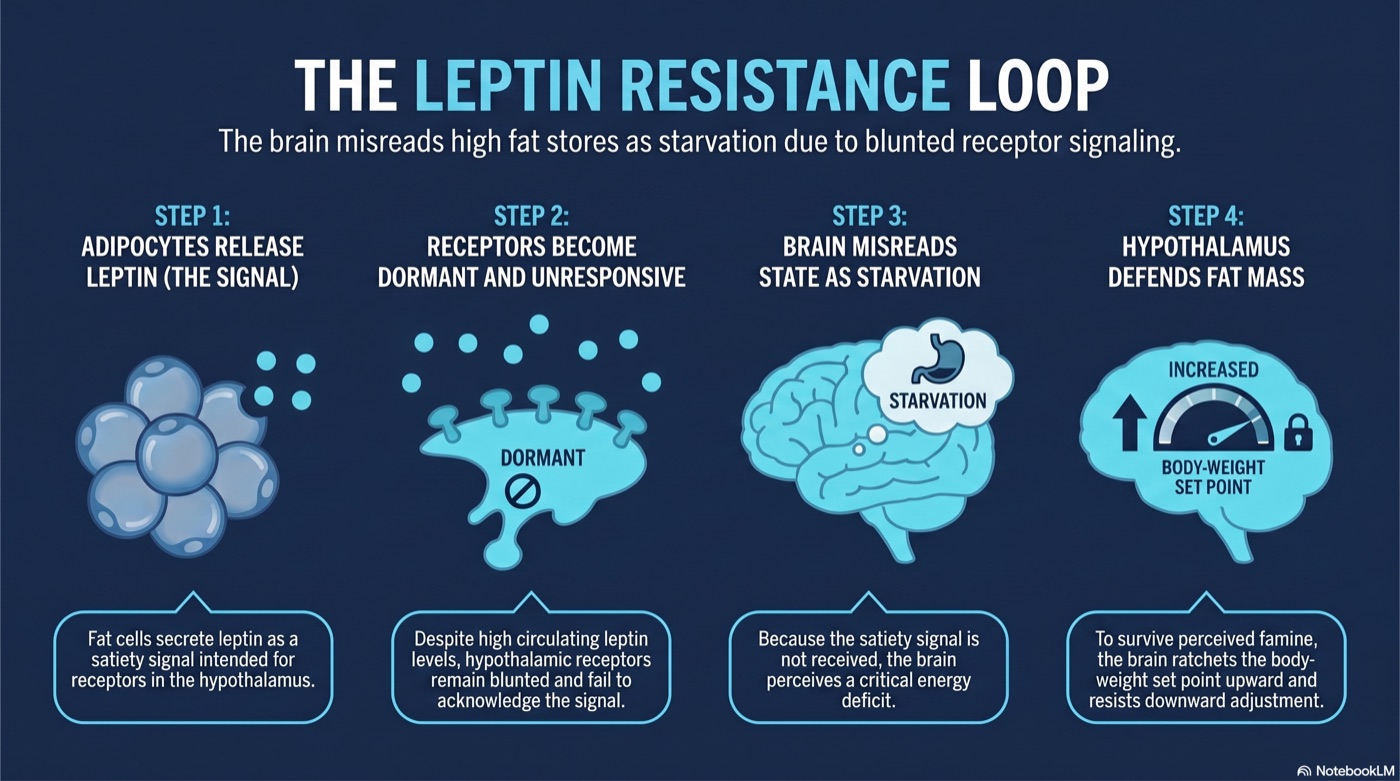
Clinical Pearl — leptin resistance. In established obesity, leptin resistance develops analogously to insulin resistance: circulating leptin concentrations are high, but the hypothalamic response is blunted. The brain perceives a state of energy deficit even when adipose stores are excessive. This is the mechanistic core of why caloric-restriction counseling alone fails for the majority of patients with established obesity — the satiety signal that should anchor portion control is not being received at full gain.
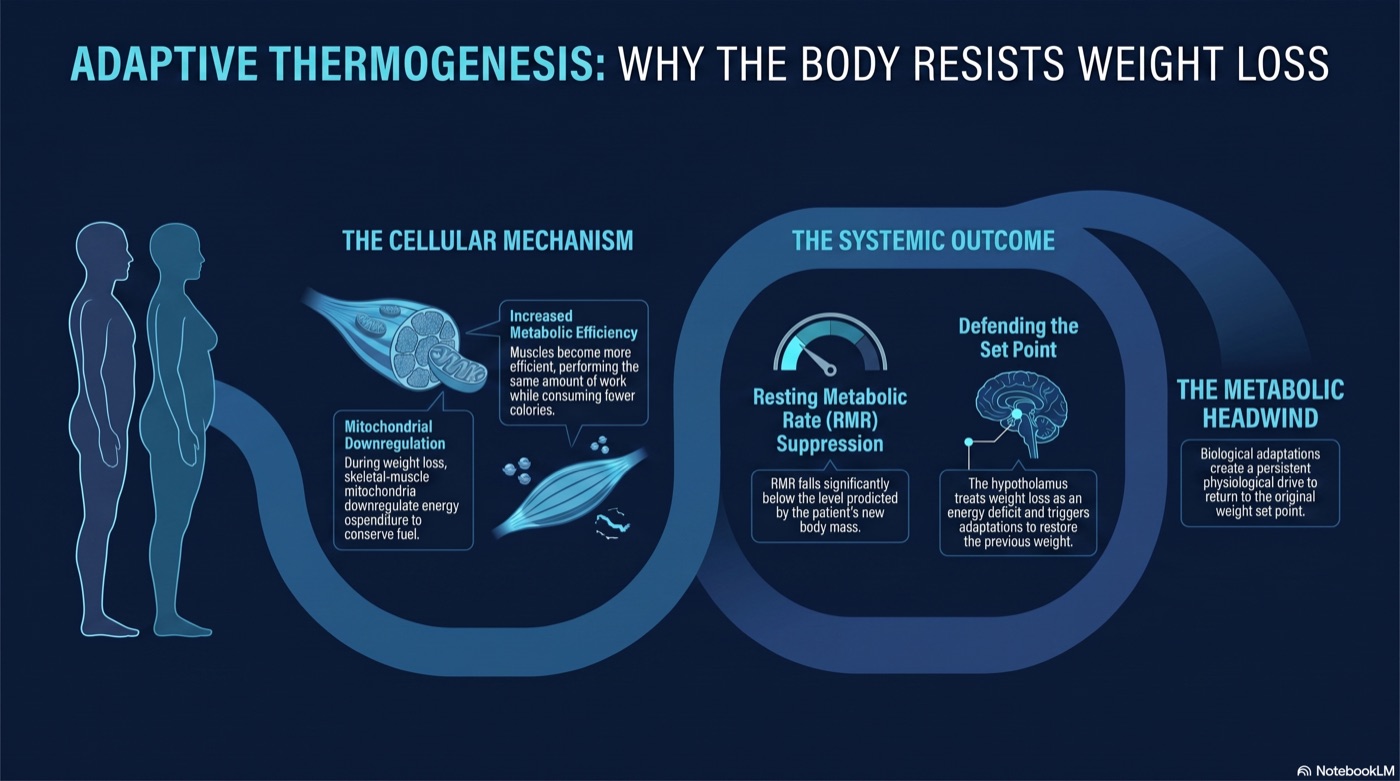
Key concept — the set-point theory. The hypothalamus defends a body-weight set point that ratchets upward with sustained caloric excess and resists downward adjustment. After weight loss through caloric restriction alone, metabolic adaptation (reduced resting metabolic rate, increased ghrelin, decreased leptin and thyroid hormones, shifts in sympathetic tone) creates a metabolic headwind that persists for years. The empirical anchor is approximately 6 kcal/kg fat-free mass/day in lean and 8 kcal/kg/day in obese subjects after 10% weight loss (Leibel 1995, PMID 7632212) — translating to roughly 300–400 kcal/day for typical patients. The Biggest Loser longitudinal cohort (Fothergill 2016, PMID 27136388) documents persistent −499 ± 207 kcal/day metabolic adaptation at 6 years post-loss. Hormonal adaptations (ghrelin elevation, leptin and PYY suppression, thyroid hormone decline) persist beyond one year of sustained loss (Sumithran 2011, PMID 22029981; Rosenbaum 2008, PMID 18842775).
Evidence — empirical anchor: Leibel RL, Rosenbaum M, Hirsch J. "Changes in energy expenditure resulting from altered body weight." N Engl J Med. 1995;332:621-628. PMID: 7632212. Original metabolic-chamber data demonstrating reductions of 6 ± 3 kcal/kg fat-free mass/day (lean) and 8 ± 5 (obese) after 10% weight loss.
Evidence — synthesis review: Rosenbaum M, Leibel RL. "Adaptive thermogenesis in humans." Int J Obes. 2010;34 Suppl 1:S47-S55. PMID: 20935667. Multi-decade synthesis establishing persistence and clinical implication.
Evidence — ≥1-year persistence (metabolic-ward demonstration): Rosenbaum M et al. "Long-term persistence of adaptive thermogenesis in subjects who have maintained a reduced body weight." Am J Clin Nutr. 2008;88:906-912. PMID: 18842775. Demonstrates metabolic adaptation persists at >1 year of sustained reduced body weight in matched-trio metabolic-ward studies.
Evidence — multi-year persistence (longitudinal cohort): Fothergill E, Guo J, Howard L, et al. "Persistent metabolic adaptation 6 years after 'The Biggest Loser' competition." Obesity (Silver Spring). 2016;24:1612-1619. PMID: 27136388. −499 ± 207 kcal/day at 6 years in 14 of 16 original contestants (P < 0.0001).
Evidence — hormonal adaptation persistence: Sumithran P, Prendergast LA, Delbridge E, et al. "Long-term persistence of hormonal adaptations to weight loss." N Engl J Med. 2011;365:1597-1604. PMID: 22029981. Ghrelin, GIP, PYY, leptin, CCK, insulin, and amylin all persistently altered in the appetite-stimulating direction at 62 weeks post-loss.
Current multi-society guidance (2025): Mozaffarian D, Agarwal M, Aggarwal M, et al. "Nutritional priorities to support GLP-1 therapy for obesity: a joint Advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society." Obesity (Silver Spring). 2025;33(8):1475-1503. PMID: 40445127. Frames metabolic adaptation after weight loss as a principal reason that pharmacologic support is the rate-limiting input for sustained loss; aligns four major societies on this position.
Section 2: Hormonal Axes Targeted by Current Pharmacotherapy (30 min)
The current and near-future pharmacopeia engages five distinct neuroendocrine axes. Understanding each axis is essential for rational protocol design — every agent in the rest of this module maps onto one or more of these axes, and clinically useful agent selection depends on knowing which axis a given patient's pathophysiology centers on.
2.1 The GLP-1 axis — GLP-1 receptor (GLP-1R) is a class B G-protein-coupled receptor expressed on pancreatic β-cells (glucose-dependent insulin secretion), pancreatic α-cells (postprandial glucagon suppression), gastric smooth muscle (delayed emptying via vagal afferents), arcuate POMC/CART neurons and brainstem NTS neurons (central appetite suppression), cardiomyocytes, vascular endothelium, and kidney epithelium. GLP-1R agonism is the single most heavily evidenced mechanism in obesity pharmacotherapy: semaglutide 2.4 mg achieves approximately −14.9% body weight at 68 weeks (STEP 1, Wilding 2021 PMID 33567185); liraglutide 3.0 mg achieves approximately −8% (SCALE, Pi-Sunyer 2015 PMID 26132939); SELECT (Lincoff 2023 PMID 37952131) established a 20% relative reduction in major adverse cardiovascular events in adults with obesity and established cardiovascular disease without diabetes. The class also delivers renal benefit (FLOW), MASH histological resolution (ESSENCE), and PAD walking-capacity improvement (STRIDE).
2.2 The GLP-1 + GIP coaxis (dual incretin) — GIP receptor (GIPR) is a class B GPCR expressed on β-cells (additive to GLP-1R for glucose-dependent insulin secretion), adipose tissue (modulates lipid handling with research-active directional question), bone, and CNS. Tirzepatide is the approved dual GLP-1/GIP coagonist; SURMOUNT-1 demonstrated −20.9% body weight at 15 mg at 72 weeks (Jastreboff 2022 PMID 35658024), and the SURMOUNT-5 head-to-head (Aronne 2025 PMID 40353578) demonstrated tirzepatide −20.2% vs semaglutide −13.7% at 72 weeks in adults with obesity without diabetes. The GIPR component appears to add weight-loss magnitude beyond GLP-1R-monotherapy at matched doses; the mechanism for GIPR-mediated weight loss (adipose lipid handling, central appetite circuits, β-cell insulin secretion potentiation, or some combination) remains an active research direction.
2.3 The GLP-1 + glucagon dual axis — Glucagon receptor (GCGR) is a class B GPCR with hepatocyte-dominant expression (drives fatty-acid β-oxidation chronically via AMPK activation and gluconeogenic enzyme transcription via cAMP/PKA/CREB), with additional expression on brown adipose tissue (thermogenesis support), kidney proximal tubule, and CNS. Survodutide (Boehringer Ingelheim / Zealand BI 456906; pre-approval-for-marketing-claims; SYNCHRONIZE-1 April 2026 sponsor topline approximately 16.6% body weight loss at 6.0 mg / 76 weeks; LIVERAGE F2/F3 + LIVERAGE-Cirrhosis F4 Phase 3 trials recruiting) is the most clinically advanced GLP-1/glucagon dual agonist. Survodutide's mechanism-class-distinctive feature is direct hepatic GCGR engagement driving fatty-acid oxidation — a mechanism single GLP-1R agonists and dual GLP-1/GIP coagonists do not engage at the receptor level. The Phase 2 MASH trial (Sanyal 2024 PMID 38847460) demonstrated 62% MASH resolution at the 6.0 mg dose vs 14% placebo at 48 weeks.
2.4 The GLP-1 + GIP + glucagon triaxis — Retatrutide (Eli Lilly LY3437943; pre-approval-for-marketing-claims; TRIUMPH Phase 3 program active) engages all three receptors with intentionally tuned activity (GIPR ~0.06 nM, GLP-1R ~0.8 nM, GCGR ~5.8 nM per Coskun 2022 PMID 35985340). The Phase 2 obesity trial (Jastreboff 2023, PMID 37366315) demonstrated −24.2% body weight at 12 mg / 48 weeks under the treatment-policy estimand. TRIUMPH-4 obesity + knee osteoarthritis Phase 3 (NCT05931367; n=445; 68 weeks; COMPLETED 2025-11-14) reached sponsor-disclosed topline December 11, 2025: −28.7% body weight reduction at 12 mg vs placebo. Regulatory-status precision: TRIUMPH-4 effect-size and safety data here are anchored to the Eli Lilly investor disclosure; peer-reviewed primary publication is pending.
2.5 The amylin axis — Amylin receptors are obligate heterodimers of the calcitonin receptor (CTR) with receptor activity-modifying proteins (RAMP1, RAMP2, RAMP3), generating three subtypes: AMY1 (CTR + RAMP1), AMY2 (CTR + RAMP2), AMY3 (CTR + RAMP3). The amylin axis is mechanistically distinct from the incretin axes — the calcitonin receptor alone has low amylin affinity; RAMP co-expression is required for high-affinity amylin binding. The dominant clinical-effect sites are the brainstem area postrema and NTS (which sit functionally outside the blood-brain barrier and are accessible to circulating amylin), with secondary sites on pancreatic α-cells (postprandial glucagon suppression independent of GLP-1R-mediated suppression), hypothalamus, kidney, bone, and brown adipose tissue. Cagrilintide (Novo Nordisk NN9838 / AM833) is the long-acting (~7-day half-life via C18 fatty-diacid acylation) amylin analog; the REDEFINE-1 cagrilintide-alone arm (Garvey 2025 NEJM, PMID 40544433) demonstrated 11.8% body weight loss at 68 weeks. Pramlintide (pramlintide; AstraZeneca, originator Amylin Pharmaceuticals) is the predecessor first-generation amylin analog — approved 2005 for T1D/T2D insulin adjunct; short half-life (~48 min); TID dosing. The amylin axis becomes load-bearing in Module 5 because it is the first non-GLP-1, non-GIP, non-glucagon mechanism class to reach Phase 3 weight-management evidence — and because cagrilintide is the active component of CagriSema, the combination product in Phase 3 regulatory submission. Mechanistic class adjacencies to monitor: the CTR component of the amylin receptor heterodimer overlaps biology with thyroid C-cell calcitonin biology (relevant to the MTC framework that emerged from rodent GLP-1 RA studies) and with osteoclast / bone-turnover biology (calcitonin's historical clinical use); cagrilintide-specific characterization in these domains is research-active.
2.6 The amylin + GLP-1 combination axis — CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg fixed-dose combination; Novo Nordisk; pre-approval-for-marketing-claims, regulatory dossier submitted) is the first combination product co-formulating two distinct mechanism classes (amylin analog + GLP-1 RA) in a single weekly subcutaneous injection. REDEFINE-1 Phase 3 (Garvey 2025 NEJM, PMID 40544433; n=3,417; 68 weeks; 4-arm: CagriSema + cagrilintide-alone + semaglutide-alone + placebo) demonstrated CagriSema 22.7% body weight loss vs cagrilintide-alone 11.8% vs semaglutide-alone 16.1% vs placebo 2.3–3.0%; the combo effect approximates the arithmetic sum of single-mechanism contributions, consistent with additive (not synergistic) mechanism integration at population scale. REDEFINE-2 (Davies 2025 NEJM, PMID 40544432; n=1,206; obesity + T2D; 2-arm placebo-controlled) demonstrated CagriSema −13.7% vs placebo −3.4% (3:1 randomization; −10.4 pp difference); placebo-controlled superiority demonstrated. The combination-product strategy is mechanistically distinct from single-molecule polyagonists (tirzepatide, retatrutide, survodutide) — same maximum-effect tier, different drug-development pathway.
2.7 The basal-insulin + GLP-1 combination axis (T2D-focused) — insulin icodec + semaglutide (Novo Nordisk insulin icodec + semaglutide combination; EMA-approved 2025-11-24 for T2D; US approval pending) is the second combination-product approach, co-formulating a once-weekly basal insulin analog (insulin icodec; approved 2024 as standalone for T2D) with semaglutide in a single weekly subcutaneous injection. insulin icodec + semaglutide is indicated for T2D glycemic control, not chronic weight management — the COMBINE 2 trial (Lingvay 2025 Diabetologia PMID 39820580) demonstrated insulin icodec + semaglutide +0.84 kg vs semaglutide −3.70 kg over 52 weeks, reflecting the insulin component's anabolic contribution. insulin icodec + semaglutide is included here because it represents the combo-product strategy applied to a different two-mechanism pair — and because the patient who needs basal-insulin replacement plus GLP-1R-mediated postprandial control is a clinically distinct population from the weight-management-focused obesity population.
2.8 The oral non-peptide GLP-1 RA platform — Orforglipron (Eli Lilly LY3502970; pre-approval-for-marketing-claims; NDA submission anticipated end of 2025 for obesity per Lilly investor disclosures) is the first oral non-peptide small-molecule GLP-1 receptor agonist to reach Phase 3 publication. ATTAIN-1 Phase 3 obesity (Wharton 2025 NEJM, PMID 40960239; n=3,127; 72 weeks) demonstrated −11.2% mean body weight reduction at the 36 mg dose vs −2.1% placebo. ATTAIN-2 obesity + T2D (Horn 2026 Lancet, PMID 41275875) extended into the obesity-with-T2D population; ACHIEVE-1 T2D (Rosenstock 2025 NEJM, PMID 40544435) established the T2D evidence base. Platform differentiation is important: orforglipron is a non-peptide spiropiperidine-based small molecule with room-temperature stability, chemical-synthesis manufacturing (vs solid-phase peptide synthesis), oral bioavailability without permeation enhancer, and dosing flexibility free of the food/water timing restrictions that constrain oral peptide GLP-1 (oral semaglutide = oral semaglutide + SNAC permeation enhancer; ≥30-min fasted dosing window required). The non-peptide chemistry confers manufacturing, supply-chain, storage, and access implications distinct from the peptide GLP-1 RA class.
2.9 The GH / IGF-1 axis (visceral and lean-mass adjuncts) — Tesamorelin is an approved (2010) GHRH analog with an on-label indication for HIV-associated lipodystrophy. The off-label use for visceral fat reduction in non-HIV populations and the use of GH secretagogues (CJC-1295/Ipamorelin, Sermorelin) for lean-mass support during weight loss are developed in M5.5 and M5.6. The mechanistic role in M5.1's scope: the GH axis becomes load-bearing for the lean-mass-preservation question that GLP-1 RA therapy creates, and for the visceral-fat phenotype where GLP-1 RA alone may not address the patient's principal concern.
2.10 The mitochondrial / NAD+ / lipolysis pathways — MOTS-c (mitochondrial-derived peptide; AMPK activation), AOD-9604 (hGH residues 177–191 fragment; lipolysis without GH effects), and 5-Amino-1MQ (NNMT inhibitor; NAD+ metabolism) are developed in M5.5 / M5.6. They are adjunctive to the principal neuroendocrine axes addressed by the GLP-1 / amylin classes; their pedagogical role is for stubborn-fat-phenotype and metabolic-flexibility contexts.
Mechanism-axis summary table (M5.1 scope; specific agent and effect-size detail in later lessons):
| Axis | Receptor pharmacology | Representative agents | Current evidence ceiling |
|---|---|---|---|
| GLP-1 (single) | GLP-1R single agonist | Semaglutide, liraglutide, orforglipron, aleniglipron | Semaglutide 2.4 mg: −14.9% (STEP 1); ATTAIN-1: −11.2% at 36 mg orforglipron |
| GLP-1 + GIP (dual incretin) | GLP-1R + GIPR coagonist | Tirzepatide | Tirzepatide 15 mg: −20.9% (SURMOUNT-1); SURMOUNT-5 −20.2% vs sema −13.7% |
| GLP-1 + glucagon (dual) | GLP-1R + GCGR coagonist | Survodutide, mazdutide | Survodutide ~16.6% at 6 mg / 76 wk (SYNCHRONIZE-1 topline) |
| GLP-1 + GIP + glucagon (triagonist) | GLP-1R + GIPR + GCGR | Retatrutide | Phase 2: −24.2% at 12 mg / 48 wk (Jastreboff 2023); TRIUMPH-4 topline: −28.7% at 12 mg / 68 wk |
| Amylin (single) | CTR + RAMP1/2/3 heterodimers | Cagrilintide, pramlintide (predecessor) | Cagrilintide 11.8% at 68 wk (REDEFINE-1 alone arm) |
| Amylin + GLP-1 (combo product) | Co-formulated amylin analog + GLP-1 RA | CagriSema | 22.7% at 68 wk (REDEFINE-1) |
| Basal insulin + GLP-1 (combo product, T2D-focused) | Insulin receptor + GLP-1R | insulin icodec + semaglutide | T2D glycemic indication; weight axis: +0.84 kg vs sema −3.70 kg (COMBINE 2) |
| Bispecific GIPR-antagonist + GLP-1R-agonist | Anti-GIPR antibody + GLP-1R agonism | MariTide (Amgen maridebart cafraglutide) | MARITIME Phase 3 obesity active; Phase 2 readouts published |
| GH / IGF-1 | GHRH-R or GHS-R | Tesamorelin (approved for HIV lipodystrophy on-label), CJC-1295/Ipamorelin, Sermorelin | Visceral / lean-mass support; M5.5 / M5.6 scope |
| Mitochondrial / NAD+ / lipolysis | AMPK, NNMT, fragment-lipolysis | MOTS-c, AOD-9604 (Frag 177-191), 5-Amino-1MQ | Adjunctive; M5.5 / M5.6 scope |
Regulatory pathway status (legal context, not evidence-quality signal):
- US-approved for chronic weight management: Semaglutide (2.4 mg and semaglutide 7.2 mg; March 2026 approval), Tirzepatide, Liraglutide, Setmelanotide (POMC/PCSK1/LEPR/Bardet-Biedl; targeted-monogenic indication).
- US-approved for adjacent indications (off-label weight-management use occurs): Tesamorelin (approved 2010 for HIV-associated lipodystrophy; off-label use for visceral fat in non-HIV populations is off-label use of an approved drug, distinct from compounded peptides).
- EMA-approved, US approval pending: insulin icodec + semaglutide (EMA-approved 2025-11-24 for T2D).
- Active Phase 3 with primary publications and US submission pending or anticipated: Retatrutide (TRIUMPH; submission anticipated post-Phase-3 program completion per Lilly disclosures), Orforglipron (NDA submission anticipated end of 2025 obesity / 2026 T2D per Lilly disclosures), Survodutide (FDA Breakthrough Therapy designation for MASH; SYNCHRONIZE-1 topline disclosed), Cagrilintide / CagriSema (Novo Nordisk regulatory dossier submitted following REDEFINE-1/-2 publications).
- Active Phase 2 → Phase 3 program anticipated: Aleniglipron (oral non-peptide GLP-1 RA; Phase 3 H2 2026 per public disclosures), MariTide (Amgen MARITIME Phase 3 obesity).
- NMPA-approved (China), US approval pending: Mazdutide (Innovent IBI362; NMPA-approved 2024 for chronic weight management).
- 503A compounding (Pharmacy Compounding Advisory Committee bulks list category-2 status; investigational profile): AOD-9604, MOTS-c, CJC-1295/Ipamorelin, Sermorelin (formerly approved as Geref, withdrawn 2008 for manufacturing reasons), 5-Amino-1MQ (non-peptide small molecule).
Regulatory status reflects commercial pathway, not science. Every informed-consent discussion with a weight-management patient should clearly identify which regulatory pathway each agent in the proposed protocol occupies, what surveillance the approved agents have undergone, and what the practitioner's clinical judgment is regarding the evidence base for any compounded or off-label component.
Section 3: Patient Phenotyping for Protocol Selection (20 min)
Effective peptide selection begins with phenotyping. Not all obesity is the same biology, and the mechanism-class taxonomy in Section 2 maps onto patient phenotypes with meaningful clinical resolution. The Acosta et al pragmatic trial in an obesity clinic (PMID 33759389; Obesity (Silver Spring) 2021;29:662-671) demonstrated that phenotype-guided selection of antiobesity medications produced 15.9% mean weight loss at 12 months versus 9.0% with non-phenotype-guided selection — a 1.75-fold difference, anchored to the four phenotypes ("hungry brain," "emotional hunger," "hungry gut," "slow burn") their group developed. The four-phenotype scheme below is the Module 5 working framework — adapted to the current mechanism-class taxonomy.
Phenotype 1: Hyperphagic / Appetite-Driven Obesity
- Primary driver: Excessive caloric intake, blunted satiety signaling at the hypothalamic/brainstem integration point
- Presentation: Constant hunger, difficulty with portion control, emotional eating, food preoccupation between meals
- Best mechanism-class targets: Single GLP-1 RA (semaglutide 2.4 mg first-line; orforglipron once approved and the patient prefers oral); dual GLP-1/GIP (tirzepatide) where greater effect size is clinically indicated; amylin-axis adjunct (cagrilintide, CagriSema when approved) where central appetite suppression remains incomplete on GLP-1 alone — the amylin axis engages a distinct receptor system that is mechanistically additive
- Lab markers: Elevated fasting insulin, elevated ghrelin-to-leptin ratio, often within otherwise unremarkable lipid panels at presentation
Phenotype 2: Metabolic / Insulin-Resistant Obesity
- Primary driver: Insulin resistance, impaired glucose disposal, visceral adiposity, often with concurrent MASLD/MASH
- Presentation: Central obesity, metabolic syndrome features, elevated HbA1c (5.7–6.4%), elevated triglycerides, low HDL, fatty liver on imaging
- Best mechanism-class targets: Dual GLP-1/GIP (tirzepatide — first-line for the insulin-resistant phenotype given the added GIPR insulin-secretory potentiation and adipose-tissue mechanism contribution); GLP-1/glucagon dual (survodutide once approved, particularly where MASH/MASLD coexists — the hepatic GCGR component drives fatty-acid β-oxidation in a way single GLP-1 RAs and dual incretins do not); triagonist (retatrutide once approved, where the full triaxis weight-loss + hepatic-fat + glycemic profile is clinically appropriate); MOTS-c as metabolic-flexibility adjunct
- Lab markers: HOMA-IR > 2.5, triglycerides > 150, fasting glucose > 100, MASLD on imaging or elevated transaminases with NAFLD pattern
Phenotype 3: Hormonal / Age-Related Obesity
- Primary driver: Declining GH/IGF-1, declining gonadal hormones (testosterone in men; estradiol in postmenopausal women), suboptimal thyroid signaling
- Presentation: Gradual weight gain with age, loss of lean mass, fatigue, reduced exercise capacity, sarcopenia features on body composition
- Best mechanism-class targets: GH-axis support (CJC-1295/Ipamorelin, Tesamorelin off-label for visceral component, Sermorelin) integrated with hormonal optimization (TRT or HRT where clinically indicated and within scope); GLP-1 RA where weight-management indication coexists, with explicit lean-mass-preservation protocol (M5.6)
- Lab markers: Low IGF-1, low free testosterone (men) or symptomatic perimenopausal-postmenopausal hormonal profile (women), suboptimal TSH/free T3, reduced lean mass on DEXA
Phenotype 4: Stubborn-Fat / Plateau Obesity
- Primary driver: Metabolic adaptation after prior weight loss; localized resistant adipose; reduced resting metabolic rate; defended set point post-induction-phase response
- Presentation: Patient can't lose "the last 10–20 lb," history of yo-yo dieting, often already on GLP-1 RA with attenuated response, may be in maintenance phase post-induction loss
- Best mechanism-class targets: AOD-9604 (localized lipolysis adjunct); MOTS-c (metabolic flexibility); GHK-Cu for post-loss skin laxity that drives discontinuation; consideration of mechanism-class switch (single GLP-1 → dual incretin → triagonist when available) where induction-phase response is inadequate
- Lab markers: Often normal glucose / insulin / lipids but reduced RMR on indirect calorimetry; loss-of-lean-mass on DEXA where preservation has been incomplete
Clinical Pearl — mixed phenotypes are the rule. Most patients present as mixed phenotypes — appetite-driven plus metabolic, or metabolic plus age-related, or post-induction with residual appetite component. The tiered approach in M5.8 (titration) allows you to address the dominant phenotype first with the appropriate mechanism class, then layer additional agents to address secondary drivers as the patient's response shape emerges over 6-12 months.
Clinical Pearl — when labs are mostly normal. When labs are mostly normal and the clinical picture is ambiguous, the default first-line for adults meeting guideline BMI/weight-related-comorbidity thresholds is a GLP-1 RA (semaglutide 2.4 mg or tirzepatide titrated to tolerance), with explicit acknowledgment to the patient that you are starting with the broadest-effect agent and will refine based on response. Family history of obesity / T2D / bariatric surgery and a self-reported "always hungry / food preoccupation" pattern are clinically actionable even when labs do not decisively point to a single phenotype.
Evidence — phenotype-guided selection: Acosta A, Camilleri M, Abu Dayyeh B, et al. "Selection of Antiobesity Medications Based on Phenotypes Enhances Weight Loss: A Pragmatic Trial in an Obesity Clinic." Obesity (Silver Spring). 2021;29(4):662-671. PMID: 33759389. 15.9% phenotype-guided vs 9.0% non-phenotype-guided at 12 months (1.75-fold).
Section 4: Why Lifestyle Alone Is Insufficient for Most Patients (15-18 min)
The evidence base on lifestyle-only weight management is one of the most studied in modern medicine, and the conclusion is consistent: durable, clinically meaningful weight loss through lifestyle modification alone is achievable for a minority of patients, and the principal reason is biology, not behavior.
The metabolic-headwind argument (revisiting Section 1).
The adaptive thermogenesis findings from Section 1 (Leibel 1995 PMID 7632212; Rosenbaum 2008 PMID 18842775; Fothergill 2016 PMID 27136388) and the hormonal-adaptation findings (Sumithran 2011 PMID 22029981) together establish a measurable, persistent, hormonally mediated reduction in energy expenditure plus an upregulation of orexigenic drive after weight loss. The adaptation is not extinguishable through willpower or "just sticking with the diet." Empirically, it has been measured at >1 year in matched-trio metabolic-ward studies (Rosenbaum 2008) and at 6 years in the Biggest Loser longitudinal cohort (Fothergill 2016).
This is the mechanistic frame for everything that follows. When a patient with a 30-pound weight loss plateaus and begins regaining despite unchanged behavior, the question is not "what did the patient do wrong?" — it is "how is the patient's biology defending against the new lower set point?" The 2025 multi-society advisory (PMID 40445127, joint statement from ACLM/ASN/OMA/TOS) names this explicitly as the principal reason that lifestyle support alone is insufficient for most patients with established obesity, and frames pharmacotherapy as the intervention that reduces the magnitude of the headwind enough to make lifestyle changes sustainable.
Key findings from landmark trials:
- Look AHEAD trial (Wing RR et al, NEJM 2013;369:145-154, PMID: 23796131; n=5,145 adults with T2D): Intensive lifestyle intervention produced 8.6% weight loss at year 1, decaying to 6.0% at study end (median 9.6 years follow-up, max 13.5 years), versus 0.7% and 3.5% in the diabetes-support-and-education control. The trial was stopped early for futility on the cardiovascular endpoint — intensive lifestyle did not reduce MACE in this population. The weight-loss curve illustrates the regain trajectory: peak response at 12 months, partial regain through years 2–4, plateau thereafter.
- DPP (Knowler WC et al, NEJM 2002;346:393-403, PMID: 11832527; n=3,234): Lifestyle intervention reduced T2D incidence by 58% (95% CI 48–66%) at average 2.8-year follow-up. Mean weight loss in the lifestyle arm was approximately 5.6 kg (≈6% body weight, from full-text Table 2) versus the protocol target of ≥7%. The intervention was effective on the diabetes-prevention endpoint but did not deliver durable, large-magnitude weight loss. Subsequent analysis (Hamman RF et al, Diabetes Care 2006;29:2102-2107, PMID: 16936160) quantified the dose-response: each 1-kg weight loss reduced diabetes incidence by 16% (HR 0.42 per 5-kg loss), establishing weight loss as the dominant predictor of risk reduction.
- STEP 1 (Wilding JPH et al, NEJM 2021;384:989-1002, PMID: 33567185; semaglutide 2.4 mg, n=1,961): −14.9% mean weight loss at 68 weeks with concurrent lifestyle intervention — approximately triple the effect size of the lifestyle-only Look AHEAD intervention at year 1.
- SURMOUNT-5 head-to-head (Aronne LJ et al, NEJM 2025, PMID: 40353578; tirzepatide vs semaglutide 2.4 mg in adults with obesity without T2D): tirzepatide −20.2% vs semaglutide −13.7% at 72 weeks. The most rigorous head-to-head direct comparison among the leading approved agents.
The "<20% sustain ≥10% loss at 5 years" claim, reframed with appropriate epistemic humility.
A common shorthand in obesity-medicine teaching is that fewer than 20% of patients sustain ≥10% weight loss at 5 years through lifestyle alone. The directional claim is well supported, but the literature is more nuanced than a single percentage suggests. The most rigorous synthesis remains Anderson JW et al (Am J Clin Nutr 2001;74:579-584, PMID: 11684524) — a meta-analysis of 29 US studies — which reported that at 4–5 years post structured lifestyle program, the average participant maintained approximately 3 kg of weight loss (~3% of initial body weight). Stratification matters: balanced hypoenergetic diets maintained only 2.0 kg (95% CI 1.5–2.5); very-low-energy diets maintained 7.1 kg (95% CI 6.1–8.1, ≈29% of initial loss). More recent narrative syntheses (Hall KD, Kahan S. Med Clin North Am 2018;102:183-197, PMID: 29156185) reinforce that the modal long-term outcome for lifestyle-only intervention is partial regain to within a few kg of baseline.
The point is not that lifestyle fails — it is that the biology defends against it, and most patients cannot indefinitely outlast that defense without pharmacologic support.
Clinical pearl — communicating "biology, not blame."
Many of your weight-management patients arrive carrying years of accumulated shame from previous failed attempts. They have been told — often by other clinicians — that they "just need to try harder," "stop snacking," or "have more discipline." This framing is wrong, and it is also clinically counterproductive: a patient who believes their weight is a moral failing is less likely to engage with chronic-disease management, and more likely to discontinue therapy when the inevitable plateaus happen.
A frame that works in clinic, condensed to language you can use directly:
"What we now understand is that obesity is a chronic neuroendocrine disease — your brain has set a higher target weight, and it defends that target with measurable changes in your metabolic rate and your hunger signaling. This is not a willpower problem. The reason previous diets stopped working was not that you failed them — it was that your biology adapted to defend the higher set point. The medications we use don't replace the work of changing how you eat and move; they reduce the size of the headwind your biology is creating, so the work you're doing actually translates into sustained loss."
This is not a soft preamble before "real" obesity care — this conversation is obesity care. Documenting it in your shared decision-making note matters both clinically (it shifts the patient frame from failure to disease management) and medico-legally (it establishes that the patient understood the chronic-disease nature of their condition before initiating long-term therapy).
Combined lifestyle + pharmacotherapy as the evidence-based standard.
Pharmacotherapy does not replace lifestyle intervention — it makes lifestyle intervention sustainable by reducing the magnitude of the metabolic headwind. The 2025 multi-society advisory (PMID 40445127) frames the relationship explicitly: GLP-1 receptor agonists (and the broader neuroendocrine pharmacotherapy class developed in Section 2) deliver the appetite suppression and metabolic-axis engagement that lets a patient maintain a calorie deficit and metabolic shift that their biology would otherwise defend against; structured nutrition, resistance training, and behavioral support during pharmacotherapy are what determine the quality of that loss — particularly the lean-mass-to-fat-mass ratio. Lean mass loss on incretin therapy is one of the most clinically consequential variables for long-term outcomes; see M5.6 (Lean Mass Preservation) for the protocol detail.
Clinical Pearl: When discussing "lifestyle vs. medication" with patients, the binary is almost always wrong. The clinically and evidentially correct frame is: medication + lifestyle, with each supporting the other — the medication makes the lifestyle change biologically achievable, and the lifestyle change determines whether the loss is healthy and sustainable. Skipping either side of that equation produces worse outcomes than running both together.
Section 5: Mechanism-Class Taxonomy + Current Guideline Consensus (25-30 min)
This section integrates the mechanism-class taxonomy from Section 2 with the guideline-consensus landscape from the three dominant professional societies. The intent is to make explicit how the Module 5 decision tree — phenotype → mechanism class → specific agent → titration — maps to ADA, AACE, and EASO consensus, and where the consensus is still catching up to the current evidence frontier.
5.1 ADA Standards of Care 2025 / 2026. The American Diabetes Association Standards of Care is updated annually. The 2025 edition endorses semaglutide 2.4 mg and tirzepatide 5–15 mg as first-line pharmacotherapy for chronic weight management in adults with BMI ≥30 (or ≥27 with a weight-related comorbidity). The 2026 edition integrates SOUL (oral semaglutide CV outcomes in T2D + ASCVD/CKD, PMID: 40162642), STRIDE (semaglutide for PAD walking capacity, Lancet 2025, PMID: 40169145), and the March 2026 semaglutide 7.2 mg approval, plus the EMA June 2025 NAION "very rare" classification for patient counseling. Full references: ADA Standards of Care 2025, ADA Standards of Care 2026.
5.2 AACE 2025 ABCD Algorithm. Nadolsky K, Garvey WT, Agarwal M, et al. "American Association of Clinical Endocrinology Consensus Statement: Algorithm for the Evaluation and Treatment of Adults with Obesity/Adiposity-Based Chronic Disease — 2025 Update." Endocr Pract 2025 Nov;31(11):1351-1394. PMID: 40956256. Advances the Adiposity-Based Chronic Disease (ABCD) paradigm: treatment intensity anchors to complication stage, not BMI alone. Stage 0 (no weight-related complication) → lifestyle first. Stage 1 (mild WRC) → GLP-1 agonist. Stage 2 (moderate-severe WRC — T2D, ASCVD, CKD, OSA, MASH) → GLP-1 or GIP/GLP-1 dual agonist at higher effective dose plus metabolic/bariatric surgery evaluation. AACE 2025 emphasizes manufacturer-supplied formulations and cautions against compounded GLP-1 products outside the shortage-list framework, citing dosing-error and counterfeit concerns.
5.3 EASO 2025 Framework. McGowan B, Ciudin A, Baker JL, Busetto L, Dicker D, et al. "Framework for the pharmacological treatment of obesity and its complications from the European Association for the Study of Obesity (EASO)." Nat Med 2025;31(10):3229-3232. PMID: 41039115. Harmonizes the European clinical-care landscape with 2024–2025 evidence (SURMOUNT, STEP extension, SELECT, SURPASS, REDEFINE). Key divergence from US guidelines: EASO formally incorporates the EMA NAION "very rare" classification and advises patient counseling on ocular symptoms; US labels (April 2026) have not adopted equivalent language.
5.4 Convergent selection logic across all three guidelines:
| Clinical priority | First-line agent | Guideline anchor |
|---|---|---|
| Maximum weight reduction, good tolerance | Tirzepatide 15 mg | ADA 2026, AACE, EASO |
| Maximum weight reduction on semaglutide base | semaglutide 7.2 mg (post-2.4 mg tolerance) | ADA 2026 |
| T2D + ASCVD | Semaglutide or Tirzepatide | ADA, AACE |
| T2D + CKD | Semaglutide | ADA, AACE, EASO (FLOW) |
| T2D + PAD (claudication) | Semaglutide 1 mg | ADA 2026 (STRIDE) |
| T2D + ASCVD/CKD, oral preferred | Oral semaglutide 14 mg | ADA 2026 (SOUL) |
| MASH/MASLD (non-cirrhotic F2-F3) | Semaglutide (ESSENCE) or Tirzepatide | ADA, AACE, EASO |
| Obesity + OSA | Tirzepatide | ADA, AACE (SURMOUNT-OSA) |
| HFpEF + obesity | Semaglutide or Tirzepatide | ADA, EASO |
5.5 Quantitative efficacy hierarchy — current Phase 3 published evidence. The cross-trial hierarchy below is anchored to direct head-to-head data where available and to placebo-controlled Phase 3 readouts otherwise. Cross-trial comparison carries caveats (population differences, follow-up length differences, estimand methodology differences) — direct head-to-head trials are the strongest comparative inputs.
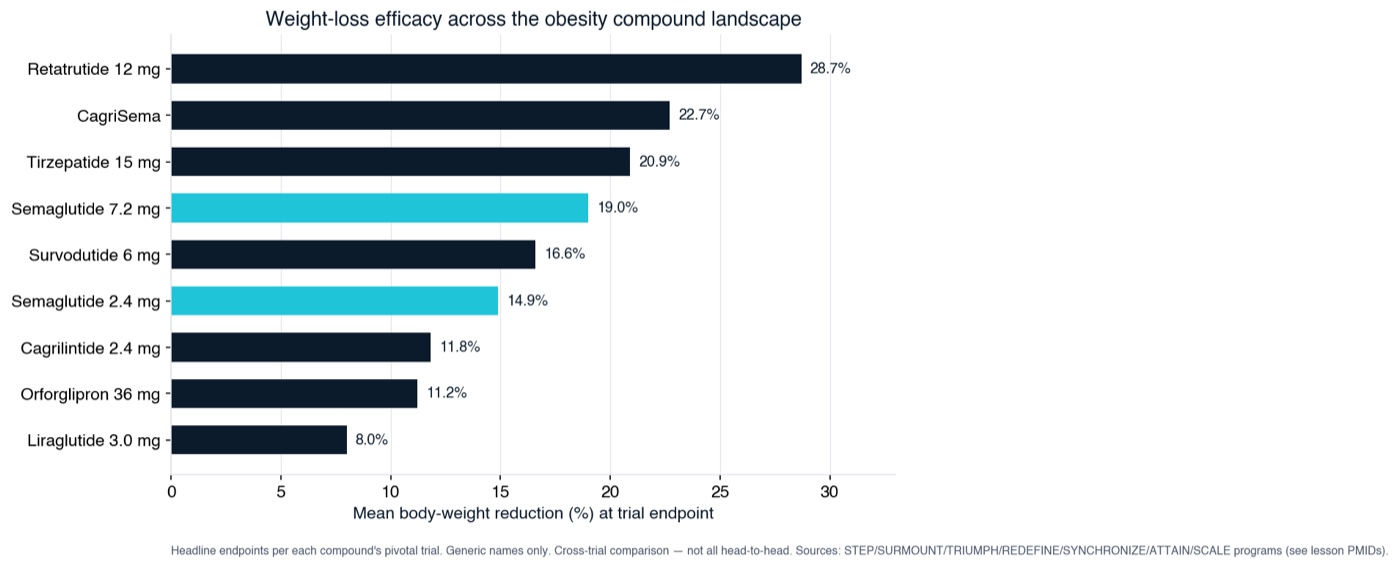
Weight-loss efficacy across the obesity compound landscape (headline trial endpoints; cross-trial, not all head-to-head; generic names).
| Mechanism class | Agent / dose | Effect size | Anchor trial |
|---|---|---|---|
| Triagonist (GLP-1/GIP/glucagon) | Retatrutide 12 mg / 68 wk | −28.7% | TRIUMPH-4 sponsor topline 2025-12-11; PMID pending |
| Amylin + GLP-1 combo | CagriSema 2.4/2.4 mg / 68 wk | −22.7% | REDEFINE-1 PMID 40544433 |
| Dual GLP-1/GIP | Tirzepatide 15 mg / 72 wk | −20.9% ITT | SURMOUNT-1 PMID 35658024 |
| Dual GLP-1/GIP (head-to-head) | Tirzepatide vs Semaglutide 2.4 mg | −20.2% vs −13.7% | SURMOUNT-5 PMID 40353578 |
| Single GLP-1 RA (high dose) | Semaglutide 7.2 mg (HD) / 72 wk | ~20.7% mean | STEP UP (approved 2026-03-19) |
| Triagonist (GLP-1/GIP/glucagon) — Phase 2 | Retatrutide 12 mg / 48 wk | −24.2% | Jastreboff 2023 PMID 37366315 |
| Dual GLP-1/glucagon | Survodutide 6.0 mg / 76 wk | ~16.6% sponsor topline | SYNCHRONIZE-1 Apr 2026; PMID pending |
| Single GLP-1 RA | Semaglutide 2.4 mg / 68 wk | −14.9% | STEP 1 PMID 33567185 |
| Amylin (alone) | Cagrilintide 2.4 mg / 68 wk | −11.8% | REDEFINE-1 cagrilintide-alone arm PMID 40544433 |
| Single GLP-1 RA (oral non-peptide) | Orforglipron 36 mg / 72 wk | −11.2% | ATTAIN-1 PMID 40960239 |
| Single GLP-1 RA (daily) | Liraglutide 3.0 mg / 56 wk | ~−8% | SCALE PMID 26132939 |
Regulatory-status precision for pre-approval agents:
- Retatrutide is already real. TRIUMPH-1 Phase 2 obesity peer-reviewed (Jastreboff 2023 NEJM); TRIUMPH-4 Phase 3 obesity + knee osteoarthritis primary-endpoint topline disclosed by Eli Lilly investor communication December 11, 2025 (−28.7% at 12 mg / 68 wk). Peer-reviewed Phase 3 primary publication is pending. The full TRIUMPH Phase 3 program (10 trials across obesity / T2D / CVD / MASLD / weight maintenance / knee OA / chronic low back pain) is enrolling or completed; regulatory submission anticipated post-Phase-3-program completion per Eli Lilly investor disclosures.
- Orforglipron is at peer-reviewed Phase 3. Three Phase 3 peer-reviewed primary publications (ACHIEVE-1 T2D PMID 40544435; ATTAIN-1 obesity PMID 40960239; ATTAIN-2 obesity + T2D PMID 41275875). NDA submission anticipated end of 2025 for obesity and 2026 for T2D per Lilly investor disclosures.
- Survodutide has SYNCHRONIZE-1 sponsor topline disclosed (April 2026: ~16.6% at 6.0 mg / 76 wk in obesity without T2D); peer-reviewed Phase 3 primary publication pending. FDA Breakthrough Therapy designation for MASH per Boehringer Ingelheim public disclosures (a regulatory-procedural designation, not approval).
- CagriSema has REDEFINE-1/-2 published (June 2025 NEJM, same-day publication, ADA 85th Scientific Sessions joint presentation); Novo Nordisk regulatory dossier submitted; submission action and approval timeline depend on the review process.
- Aleniglipron is Phase 2 → Phase 3 anticipated H2 2026 per public disclosures; not yet at Phase 3 peer-reviewed publication.
- MariTide (Amgen maridebart cafraglutide; bispecific anti-GIPR antibody + GLP-1R agonist conjugate) is in MARITIME Phase 3 obesity program. Phase 2 readouts published. The bispecific-class strategy antagonizes GIPR — the inverse-direction GIPR bet from the tirzepatide-class and retatrutide-class agonist strategies.
- Mazdutide (Innovent IBI362; GLP-1/glucagon dual agonist; same mechanism class as survodutide) is NMPA-approved (China) 2024 for chronic weight management; US approval pending.
The cross-class comparative landscape is in active evolution. The mechanism-class taxonomy from Section 2 is the durable analytical frame; effect-size rankings will shift as Phase 3 readouts mature across the triagonist, dual GLP-1/glucagon, amylin, and combo-product classes.
Section 6: Active Research Directions, Safety Class-Differentiation, and Open Questions
Honest research-education names what is established, what is class-level consensus, and what is actively under research. The following are the principal active research directions in the obesity-pharmacotherapy field. None of these are reasons to withhold appropriate treatment from patients who meet guideline criteria — they are the dimensions where clinical judgment operates ahead of definitive long-horizon RCT evidence, and where patient counseling should reflect research-state precision rather than false certainty.
6.1 Long-term GLP-1 use beyond ~5 years.
The landmark RCTs of GLP-1 receptor agonists in obesity have follow-up between 68 weeks (STEP 1, SURMOUNT-1) and approximately three to four years (SELECT extension, SUSTAIN-6 long-term follow-up). Continuous-use data beyond five years come from extension-study cohorts and registry data, both of which have selection bias — patients who tolerate and respond well are the ones who remain on therapy. The realistic clinical population is patients who will be on these agents for a decade or more, and the field does not yet have RCT-level data that maps cleanly onto that duration. Current evidence supports continued use as long as benefit-risk remains favorable; long-term cardiovascular and oncologic surveillance data continue to mature across the SELECT extension, FLOW extension, and the Phase 3 outcomes programs for the dual-agonist class (tirzepatide SURMOUNT-MMO — labeled for CWM with CV outcomes readout pending), the triagonist class (retatrutide TRIUMPH-Outcomes — investigational), and the dual GLP-1/glucagon class (survodutide SYNCHRONIZE-CVOT — investigational).
6.2 Lean-mass dynamics on incretin therapy.
The literature on lean-mass changes during incretin therapy is research-active and partially conflicting. Findings vary by measurement modality (DEXA vs MRI vs bioelectrical impedance vs proxy measures from non-DEXA trials), by trial design (whether resistance training was protocolized), and by population (older vs younger, sarcopenic vs non-sarcopenic at baseline). Practitioner experience supports resistance training plus adequate protein (≥1.2–1.6 g/kg of reference body weight) as substantially mitigating the lean-mass loss seen in lifestyle-only trial protocols; RCT-level evidence on optimal mitigation strategies is still developing. See M5.6 (Lean Mass Preservation) for the adjunctive protocol stack — including the GH-axis adjunct evidence base for CJC-1295/Ipamorelin and MOTS-c (Level III–IV mechanism + practitioner-experience anchoring).
6.3 Discontinuation and tapering strategies.
Published guidance on optimal discontinuation of GLP-1 therapy is sparse. The weight-regain trajectory after abrupt discontinuation is well documented (STEP 1 extension — Wilding 2022 PMID 35441470 — regain of approximately two-thirds of lost weight within 12 months; SURMOUNT-4 — substantial regain on continued vs withdrawal arms), but the optimal management strategy is not. Tapering protocols, maintenance-dose strategies (continuing at the lowest effective dose long-term), bridge strategies to alternative agents, and the role of intermittent dosing are all areas where practitioner experience exceeds RCT evidence. TRIUMPH-6 (retatrutide weight-reduction maintenance Phase 3; NCT06859268; primary completion 2028-04) is one of several Phase 3 trials in active development specifically addressing the maintenance-phase question.
6.4 Pediatric and adolescent use.
Expanded approvals for adolescent obesity have been granted (semaglutide ≥12 years, December 2022, based on STEP TEENS, PMID: 36322838; tirzepatide adolescent indication progressing through SURMOUNT-ADOLESCENTS). Long-term developmental and metabolic-programming considerations of multi-decade use beginning in adolescence are research-active and will require longitudinal cohort follow-up that is only just beginning. Family dynamics, shared decision-making with the adolescent and parent/guardian, and developmentally appropriate consent processes are clinical-practice-pattern domains, not evidence-prescriptive at present.
6.5 Combination therapy long-term safety.
Most clinical use of combination peptide therapy (GLP-1 + GH secretagogue, GLP-1 + AOD-9604, GLP-1 + MOTS-c) is anchored in mechanistic rationale and practitioner experience, not multi-year RCT data. The approved fixed-dose combination products (CagriSema if approved; insulin icodec + semaglutide for T2D in EMA jurisdictions) are mechanistically distinct from off-label compounded combinations — they carry trial-level safety data for the specific co-formulation. Pharmacovigilance for the compounded combination protocols is sparse relative to the surveillance infrastructure for approved drugs. This is not a reason to forgo combination protocols where clinical judgment supports them — it is a reason to document indication carefully, monitor closely, and communicate the evidence-base research-state to patients during informed consent.
6.6 NAION (non-arteritic anterior ischemic optic neuropathy) and ophthalmologic considerations.
The European Medicines Agency (EMA) classified NAION as a "very rare" adverse event of semaglutide in June 2025 and updated EU labeling accordingly. US labeling has not adopted equivalent language as of April 2026. The original signal originated in observational data (the Mass Eye and Ear cohort, JAMA Ophthalmol 2024) and has subsequently been characterized in pharmacovigilance studies — most notably Lakhani M et al. "Association of Glucagon-Like Peptide-1 Receptor Agonists With Optic Nerve and Retinal Adverse Events: A Population-Based Observational Study Across 180 Countries." Am J Ophthalmol 2025 Sept (PMID: 40383360) — which reports significantly higher odds of ischemic optic neuropathy with semaglutide (ROR 11.12 in one database; 68.58 in another) and calls for global pharmacovigilance and post-marketing surveillance. Direction-of-effect: Lakhani 2025 reports a positive ION signal with semaglutide.
Class-differentiation note. The NAION signal has been characterized for semaglutide in the published literature; an equivalent threshold-level positive signal has not been characterized for tirzepatide in the same pharmacovigilance datasets. The class-differentiation should be read with an exposure-window asymmetry caveat — semaglutide has substantially longer post-marketing exposure (approved 2017 for T2D; 2021 for chronic weight management) than tirzepatide (2022 for T2D; 2023 for chronic weight management), so the absence of a same-magnitude tirzepatide signal at the same surveillance threshold may reflect lower cumulative person-year exposure rather than a true mechanism-level class differentiation. Surveillance is ongoing.
Counseling priority. Per analysis of clinician and patient community discussions, the May 2025 EMA labeling change and subsequent media coverage produced a patient awareness wave that arrived ahead of consolidated clinician training. Patients are asking about NAION risk regardless of which label position your jurisdiction follows. The clinically appropriate response is direct counseling: (a) acknowledge NAION as a recognized but very rare adverse event associated with semaglutide; (b) contextualize the absolute risk per the EMA "very rare" classification (~1 case per 10,000 person-years order of magnitude); (c) identify the relevant patient-level risk factors (diabetes, obstructive sleep apnea, small optic disc anatomy where known) and how they shift individual risk-benefit framing; (d) establish a clear when-to-seek-care threshold — sudden vision changes or painless monocular vision loss warrant same-day ophthalmology evaluation. Detailed counseling guidance, patient-language scripts, and risk-factor-specific shared-decision-making framing live in M5.2 (Semaglutide Deep Dive). M5.1's role is to flag NAION as a counseling priority and orient the practitioner on the class-differentiation and exposure-window caveat.
6.7 Cancer surveillance — research-state synthesis and class-differentiation.
The cancer-context safety question for the GLP-1 RA class arises from rodent C-cell mechanism findings (medullary thyroid C-cell signal characterized in Bjerre Knudsen 2010), from systematic-review-level synthesis across cancer contexts, and from compound-class-specific mechanism considerations. The current Phase 3 evidence + post-marketing surveillance + meta-analytic synthesis state is more nuanced than a single yes/no answer:
- 2026 cancer SR + meta-analysis — Ko A, Chang YC, Bahar F, et al. "Risk for Cancer With Glucagon-Like Peptide-1 Receptor Agonists and Dual Agonists: A Systematic Review and Meta-analysis." Ann Intern Med 2026 Feb; epub 2025-12-09. PMID: 41359966. 48 RCTs, n=94,245; moderate-certainty evidence that GLP-1 receptor agonists and dual agonists "probably have little or no effect on risk for thyroid cancer" and similar minimal effects on pancreatic, breast, and kidney cancers (moderate certainty); other obesity-related cancers uncertain or low certainty. Authors note short trial follow-up periods and that included trials were not specifically designed to evaluate cancer outcomes. The SR reports a "little or no effect" finding with explicit certainty-tier framing.
- Bezin 2023 thyroid cancer database study — Bezin J et al. "GLP-1 Receptor Agonists and the Risk of Thyroid Cancer." Diabetes Care 2023;46:384-390. PMID: 36356111. French nationwide case-control: aHR 1.58 (95% CI 1.27–1.95) for all thyroid cancer and aHR 1.78 (95% CI 1.04–3.05) for medullary thyroid cancer for 1–3 years of GLP-1 RA use. The Bezin 2023 finding is a positive thyroid-cancer association in a specific national database that has not been consistently reproduced in subsequent cohort studies and is contextualized by the Ko 2026 meta-analytic synthesis (PMID 41359966) reporting "little or no effect" with moderate certainty across 94,245 patients. The Cancer Safety Matrix vault reference frames this accurately: Bezin reports an increased thyroid-cancer signal in the French database; the broader meta-analytic synthesis does not confirm an overall increased risk.
- MTC / MEN2 absolute contraindication remains. The class-label boxed warning on MTC and MEN2 family history is anchored in the rodent C-cell hyperplasia + tumor signal (Bjerre Knudsen 2010). Patients with personal or first-degree-relative history of MTC or MEN2 should not receive GLP-1 RAs.
- Pancreatitis + pancreatic cancer. Wen J, Nadora D, Bernstein E, et al. "Evaluating the Rates of Pancreatitis and Pancreatic Cancer Among GLP-1 Receptor Agonists: A Systematic Review and Meta-Analysis of Randomised Controlled Trials." Endocrinol Diabetes Metab 2025. PMID: 40988099. 62 RCTs, n=66,232; pancreatitis RR 1.44 (95% CI 1.09–1.89) — a 44% relative-risk elevation. Pancreatic cancer overall RR 1.30 (95% CI 0.86–1.97; non-significant); subgroup analysis with background medications showed RR 1.85 (95% CI 1.05–3.26). The class label carries a pancreatitis warning; standard practice is to discontinue if acute pancreatitis develops during use. Wen 2025 reports a positive pancreatitis signal with significance.
- Psychiatric safety. Bezin J, Bénard-Laribière A, Hucteau E, et al. "Suicide and suicide attempt in users of GLP-1 receptor agonists: a nationwide case-time-control study." EClinicalMedicine 2024;79:103017 (Feb 2025 collection). PMID: 39844933. French nationwide case-time-control: OR 0.62 (95% CI 0.51–0.75) — a protective association. Authors conclude the study "provides reassurance about the short-term psychiatric safety of GLP-1 RA." DPP-4 inhibitor negative control showed similar OR 0.75. The 2023–2024 black-box psychiatric concern that emerged from early FAERS signals has not been confirmed in the most rigorous database analyses; the protective association in Bezin 2024 is the strongest current data point on psychiatric safety — not a "weak signal of concern."
The cancer-and-safety synthesis: the boxed warning on MTC/MEN2 is absolute; the meta-analytic state across thyroid, pancreatic, breast, and kidney cancers is "little or no effect" with moderate certainty (Ko 2026); the pancreatitis class signal is real and warrants discontinuation if acute pancreatitis develops; the 2023–2024 psychiatric concern has not been confirmed and the most rigorous database analysis (Bezin 2024) reports a protective association.
6.8 Mechanism-class effect-size frontier.
The published Phase 3 effect-size ceiling has moved approximately as follows over five years: liraglutide 3.0 mg ~8% (SCALE 2015) → semaglutide 2.4 mg ~15% (STEP 1 2021) → tirzepatide 15 mg ~21% (SURMOUNT-1 2022) → tirzepatide vs semaglutide head-to-head 20.2% vs 13.7% (SURMOUNT-5 2025) → semaglutide HD 7.2 mg ~20.7% (STEP UP 2026) → CagriSema 22.7% (REDEFINE-1 2025) → retatrutide TRIUMPH-4 topline 28.7% (sponsor disclosure 2025-12-11; PMID pending). Whether the −28% to −30% retatrutide effect-size range will translate from the TRIUMPH-4 topline into the broader TRIUMPH-1/-2/-3 Phase 3 readouts in 2026-2027 — and where the bispecific MariTide and the triagonist class as a whole settle in published Phase 3 effect size — is the dominant research-frontier question of the next 24 months. The mechanism-class taxonomy in Section 2 is the durable analytical frame; specific effect-size rankings will shift across the next reporting cycles.
Section 7: Common Clinical Questions
The following questions are drawn from the recurrent issues that arise in the first 90 days of obesity-pharmacotherapy practice. Each is answered as the question would be answered to a colleague — direct, evidence-cited, practical — rather than as a textbook entry. The questions present facts and invite shared decision-making; they do not steer clinical decisions.
Q1: A patient asks if obesity is genetic — how do I answer that with current evidence?
Twin and adoption studies estimate the heritability of BMI at approximately 40–70%, comparable to height and substantially higher than most chronic diseases. The vast majority of common obesity is polygenic — hundreds of identified loci each contributing a small effect, captured in polygenic risk scores that explain a meaningful but limited fraction of population variance. Monogenic obesity is rare but clinically important: leptin and leptin-receptor mutations, MC4R mutations (the most common monogenic cause, ~2–3% of severe early-onset obesity), POMC mutations, and the syndromic forms (Bardet-Biedl, Prader-Willi). Setmelanotide (approved for POMC, PCSK1, LEPR, and Bardet-Biedl deficiencies) is the targeted therapy for select monogenic forms.
The practical patient communication: "Yes, obesity has a strong genetic component — about 40 to 70 percent of the variation in body weight between people is genetic. That doesn't mean it's destiny, and it doesn't mean treatment doesn't work. What it does mean is that the response to lifestyle alone will be highly variable from person to person, and the patients who need pharmacologic support to achieve and maintain a healthy weight are not failing — they are genetically predisposed to higher set points that respond well to the medications we have."
Evidence: Loos RJ, Yeo GS. "The genetics of obesity: from discovery to biology." Nat Rev Genet. 2022;23:120-133. PMID: 34556834.
Q2: What do I tell a patient who "doesn't believe" in the chronic disease model of obesity?
This is a patient-communication problem, not an argument to win. Motivational-interviewing principles apply directly: meet the patient where they are, ask what they have tried, what worked and what didn't, and what they hope treatment can do. Then, rather than asserting the chronic-disease model, demonstrate it from their own history — the regain after every successful diet, the hunger that returned, the way the weight crept back even when behavior didn't change. Most patients who initially resist the chronic-disease framing have experienced exactly this pattern; they have just never been given the biological framework that explains it.
Once the patient sees their own history through a different lens, the chronic-disease conversation becomes their conclusion, not yours. This conversation is obesity care — not preliminary to it. Document the shared decision-making explicitly: what the patient understands about chronic-disease management, expected duration of therapy, and the rationale for combined pharmacotherapy + lifestyle. This documentation matters clinically and medico-legally.
If the patient still does not accept the chronic-disease model after this conversation, that is their decision — but it is also a clinical signal that long-term adherence may be poor, and the treatment plan should account for that (e.g., shorter monitoring intervals, earlier reassessment of fit).
Evidence: Rollnick S, Miller WR, Butler CC. "Motivational Interviewing in Health Care," 2nd ed. Guilford 2022. Practitioner-expert-consensus reference (Level IV).
Q3: How do I phenotype a patient when their labs are mostly normal?
The four-phenotype framework in Section 3 is explicitly probabilistic — most patients present as mixed, and labs do not always decisively point to one driver. When labs are mostly normal and the clinical picture is ambiguous, weight the following:
- Weight gain pattern. Childhood-onset and steady through life suggests genetic / set-point-anchored phenotype (Phenotype 1). Adult-onset post-pregnancy, post-medication, post-job-change suggests environmental / behavioral overlay. Gradual age-related gain with energy decline suggests Phenotype 3 even when labs are borderline.
- Family history. First-degree relatives with obesity, T2D, or bariatric history substantially raises pre-test probability of metabolic / set-point-defended obesity that will benefit from incretin first-line.
- Hunger and satiety self-report. "I'm always hungry / I never feel full / I think about food constantly" maps to Phenotype 1 — this self-report is clinically actionable even when labs are normal, and these patients respond well to GLP-1 RAs.
- Body composition rather than BMI. Visceral-predominant adiposity on exam (waist circumference > 102 cm men / > 88 cm women, or waist-to-height ratio > 0.5) suggests metabolic phenotype even with normal HbA1c.
When uncertain, the default first-line for most adults meeting guideline BMI/WRC thresholds is a GLP-1 RA (semaglutide 2.4 mg or tirzepatide titrated to tolerance), with the explicit acknowledgment to the patient that you are starting with the broadest-effect agent and will refine based on response. This is consistent with ADA 2025/2026 and AACE 2025.
Evidence: Acosta A et al. "Selection of Antiobesity Medications Based on Phenotypes Enhances Weight Loss." Obesity (Silver Spring). 2021;29(4):662-671. PMID: 33759389.
Q4: A patient asks "do I have to be on this forever?" — how do I answer?
The honest answer is: probably long-term, possibly indefinitely, and we will reassess together at intervals. Obesity is a chronic disease; the medications work while you take them, and the underlying biology — the defended set point, the metabolic adaptation, the hormonal headwind documented in Sumithran 2011 (PMID 22029981) — does not resolve when the medication stops. The STEP 1 extension and SURMOUNT-4 data both show substantial weight regain within 12 months of discontinuation in the majority of patients, which is consistent with the set-point biology you walked through earlier in the lesson.
That said, indefinite is not the only model. Some patients will do well on a maintenance dose lower than their induction dose. Some will tolerate intermittent or seasonal dosing with adequate behavioral support. Some patients may eventually transition off pharmacotherapy if they have achieved sustained metabolic improvement and are willing to accept higher monitoring intensity for early signs of regain. The optimal strategy is individualized and the evidence base is genuinely thin (see Section 6.3). The TRIUMPH-6 retatrutide weight-maintenance Phase 3 trial (NCT06859268; primary completion 2028-04) is one of several Phase 3 trials specifically addressing the maintenance question.
The frame that works in clinic: "We treat obesity the way we treat hypertension or hyperlipidemia — with chronic medication, ongoing lifestyle support, and regular reassessment. We do not stop blood pressure medication when the blood pressure is controlled and call that a cure. The medication is doing what your biology cannot do on its own. If at some point your situation changes and we can step down or discontinue, we will reassess together — but we should plan as though this is a long-term partnership, not a short-term diet."
Evidence: Wilding JPH et al. STEP 1 extension. Diabetes Obes Metab. 2022;24:1553-1564. PMID: 35441470.
Q5: A patient is concerned about thyroid cancer risk on semaglutide or tirzepatide — what do I tell them?
The concern derives from the class-label boxed warning on GLP-1 receptor agonists for medullary thyroid carcinoma (MTC) and multiple endocrine neoplasia syndrome type 2 (MEN2). The warning is based on rodent data — rat C-cell hyperplasia and tumors in chronic exposure studies (Bjerre Knudsen 2010, PMID 20203154) — and rats have a substantially different thyroid C-cell physiology than humans.
The clinical bright lines:
- MTC personal or family history → absolute contraindication. Do not prescribe.
- MEN2 personal or family history → absolute contraindication. Do not prescribe.
- Routine elevated calcitonin screening → not currently recommended by major society guidelines; the test is poorly performant in this context (low specificity, high false-positive rate).
- Papillary thyroid cancer (the most common form of thyroid cancer in the US) is a different entity and is not contraindicated by the boxed warning. If the patient has personal history of papillary thyroid cancer, GLP-1 RAs are not contraindicated; the discussion is around general oncology surveillance, not an MTC-specific concern.
The current evidence synthesis state is more nuanced than a simple "yes/no" signal:
- The 2026 systematic review and meta-analysis (Ko A et al, Ann Intern Med 2026, PMID 41359966; 48 RCTs, n=94,245) reports that GLP-1 receptor agonists and dual agonists "probably have little or no effect on risk for thyroid cancer" with moderate-certainty evidence, and similar minimal effects on pancreatic, breast, and kidney cancers. Authors note short trial follow-up and that trials were not specifically designed to evaluate cancer outcomes.
- Bezin J et al, Diabetes Care 2023 (PMID 36356111) — French nationwide case-control — reports an increased thyroid cancer signal (aHR 1.58 all thyroid; aHR 1.78 medullary) for 1–3 years of GLP-1 RA use. This is the strongest published positive thyroid-cancer signal and has not been consistently reproduced in subsequent cohort studies and meta-analyses.
The patient communication: "There's a boxed safety warning based on rodent studies of a specific rare thyroid cancer called medullary. If you or any first-degree relative has a history of that specific cancer or of MEN2 syndrome, this medication is not for you. Outside that history, the strongest current evidence — a meta-analysis of 48 trials and 94,000 patients published in Annals of Internal Medicine — concludes the medications probably have little or no effect on thyroid cancer risk, with moderate certainty. A French database study did report an increased thyroid signal, which is one reason surveillance continues. The overall picture remains reassuring for patients without MTC or MEN2 history."
Evidence: Ko A et al, Ann Intern Med 2026 [PMID 41359966]; Bezin J et al, Diabetes Care 2023 [PMID 36356111]; Bjerre Knudsen L et al, Endocrinology 2010 [PMID 20203154].
Q6: Can I prescribe semaglutide off-label for weight loss in a non-diabetic patient with BMI 28 and metabolic syndrome features?
Yes — and the framing matters. The on-label indication for semaglutide weight management (semaglutide) is BMI ≥30, or ≥27 with at least one weight-related comorbidity (T2D, hypertension, dyslipidemia, OSA, ASCVD). A patient with BMI 28 and metabolic syndrome features (e.g., elevated waist circumference, low HDL, elevated triglycerides, elevated fasting glucose, elevated blood pressure — meeting NCEP/ATP-III criteria) meets the on-label indication because metabolic syndrome elements are weight-related comorbidities. This is on-label, not off-label.
If the patient is BMI 25–26 without comorbidity, prescribing falls into off-label territory. Off-label prescribing of approved drugs is legal and clinically common where evidence supports it. The AACE 2025 ABCD framework (Nadolsky/Garvey, PMID 40956256) anchors treatment to complication stage rather than BMI alone, which provides explicit consensus support for using BMI as one input among several rather than the gating criterion.
Documentation that protects the practice: record the specific weight-related comorbidities you are treating, the failed lifestyle trial(s) where applicable, the shared decision-making on benefit-risk, and the patient's understanding of the indication. Prior authorization realities: commercial payors increasingly require BMI ≥30 and documentation of failed lifestyle, which can constrain the practical accessibility of on-label use even where clinical indication is clear. Cash-pay practices and HSA/FSA-funded scripts have more flexibility.
Evidence: Nadolsky K, Garvey WT et al. AACE 2025 ABCD Algorithm. Endocr Pract. 2025;31(11):1351-1394. PMID: 40956256.
Q7: My patient is using compounded semaglutide from an online provider. How do I talk through it with them?
Compounded semaglutide is a real-world clinical option that emerged during the 2022–2024 FDA-declared shortage periods and continues in patient-specific contexts. The framework for the conversation:
The regulatory landscape (US, current as of April 2026):
- 503A pharmacies (state-licensed compounding pharmacies) compound for individual patients pursuant to a valid prescription. They are regulated by state boards of pharmacy, with standards for sterility, potency assays, and impurity profiles that vary across pharmacies.
- 503B outsourcing facilities are federally registered, hold themselves to higher manufacturing standards, and undergo periodic federal inspection.
- Shortage-list status timeline:
- Tirzepatide: removed from shortage list October 3, 2024; declaratory order December 19, 2024. 503A enforcement discretion ended February 18, 2025; 503B ended March 19, 2025.
- Semaglutide: removed from shortage list February 21, 2025. 503A enforcement discretion ended April 22, 2025; 503B ended May 22, 2025.
Compounding semaglutide or tirzepatide outside of patient-specific clinical-need scenarios is no longer within enforcement discretion. Patient-specific 503A compounding remains possible with documented medical necessity (e.g., excipient allergy, established clinical need that the manufacturer-supplied product cannot satisfy).
- "Online providers" sourcing from compounding pharmacies vary widely in clinical oversight, prescriber-of-record practices, and adherence to dose-titration protocols.
Operational characteristics of compounded preparations (factual scope, not deficit framing):
- Lyophilized vial format requiring reconstitution by the patient at point of use (vs the manufacturer-supplied pre-filled pen format)
- Reconstitution protocols include bacteriostatic water with measured-dose drawing technique using insulin syringe
- Storage: reconstituted preparations stable at 2–8°C for approximately 28 days vs the manufacturer-supplied pen's room-temperature stability for 56 days after first use
- Excipient profile per pharmacy specification
- Manufacturing oversight: state board of pharmacy (503A) or federal cGMP inspection (503B) vs the NDA-approved manufacturing standard for the branded semaglutide product
Quality criteria clinicians evaluate when selecting compounding pharmacies:
- Sterility testing per USP <797> and <800>
- Per-batch certificate of analysis (peptide content, purity, residual solvents, endotoxin)
- Cold-chain shipping verification
- State licensure / 503B federal registration verification
- Accreditation status (e.g., PCAB)
Patient-counseling beat:
"Compounded semaglutide is a real clinical option used by many patients. The operational differences from the manufacturer-supplied semaglutide product are real — different format that requires reconstitution at home, different oversight pathway, different storage. Costs are typically lower; the patient self-administration is similar to insulin self-injection. If you are considering continuing on a compounded preparation, let's review your specific compounding pharmacy's quality practices — sterility testing, certificate of analysis, accreditation — and walk through reconstitution technique together. That's how the decision gets made well, with eyes open to both the operational characteristics and the post-shortage regulatory landscape."
The AACE 2025 statement (Nadolsky/Garvey, PMID 40956256) emphasizes manufacturer-supplied formulations and notes manufacturing-oversight differences in the post-shortage period. Patient-specific 503A compounding with documented medical necessity remains a clinical option; the conversation with the patient is shared decision-making about quality criteria, operational characteristics, cost, and the practitioner-of-record relationship.
Evidence: AACE 2025 Algorithm — Nadolsky K, Garvey WT et al, Endocr Pract 2025;31(11):1351-1394, PMID 40956256.
Clinical pearl — self-injection is a routine clinical skill, not a barrier. The most common patient question at GLP-1 RA initiation is dose-titration tolerance — GI effects, dose-escalation cadence, and side-effect management — not the injection mechanics themselves. Self-injection is taught daily for insulin, fertility hormones, biologics, and weekly GLP-1 RA therapeutics. The needle gauge is fine (typically 29-32G for SubQ); the depth is subcutaneous (skin-deep, not muscle); the technique is demonstrated in one clinical visit and refined over the first few self-administrations. Pre-filled auto-injector pens (semaglutide, semaglutide, tirzepatide, liraglutide) further reduce procedural complexity — the patient clicks a button, the dose is pre-measured, the needle retracts. For compounded preparations, the technique adds reconstitution discipline and drawing technique with an insulin syringe — also a routine clinical skill, demonstrated in the same initiation visit. Framing self-injection as "scary," "daunting," "intimidating," or a major barrier mischaracterizes the actual patient experience once the technique is demonstrated. Counsel patients factually about technique; do not pre-load the mechanics with anxiety-coded vocabulary. The substantive practical question in titration management is dose-tolerance, not injection technique.
Q8: Which investigational Phase 3 agent should I be tracking for my insulin-resistant / MASH patient?
The two agents in active Phase 3 that map most directly onto the insulin-resistant / MASH phenotype are survodutide (GLP-1/glucagon dual agonist; hepatic GCGR engagement drives fatty-acid β-oxidation; FDA Breakthrough Therapy designation for MASH; SYNCHRONIZE-1 obesity topline April 2026 ~16.6% at 6 mg / 76 wk; LIVERAGE F2/F3 and LIVERAGE-Cirrhosis F4 Phase 3 trials recruiting) and retatrutide (GLP-1/GIP/glucagon triagonist; Phase 2 MASLD substudy demonstrated ~82% relative MRI-PDFF reduction at 12 mg / 48 wk per Sanyal 2024 PMID 38858523; TRIUMPH-4 obesity + knee OA topline 28.7% at 12 mg / 68 wk per Lilly disclosure December 2025). Both are currently pre-approval-for-marketing-claims; both have regulatory submission pathways in active progress.
For the MASH-with-cirrhosis (F4) population specifically, the LIVERAGE-Cirrhosis trial will be the first Phase 3 readout for a GLP-1/glucagon dual agonist in compensated cirrhosis. The class-comparator context is the Loomba 2023 semaglutide Phase 2 cirrhosis trial (PMID 36934740) which did not demonstrate statistically significant fibrosis improvement in the F4 cirrhosis population — establishing the mechanism-stage question of whether hepatic GCGR engagement (survodutide, retatrutide) will outperform GLP-1R-only mechanism in the cirrhosis population. The mechanism rationale supports a hypothesis of direct hepatic GCGR-mediated benefit beyond weight-loss-mediated effect; the Phase 3 readouts will adjudicate.
For non-cirrhotic MASH F2/F3, the current approved options are resmetirom (Madrigal; thyroid hormone receptor-β agonist; approved 2024) and semaglutide (ESSENCE trial — Sanyal AJ, Newsome PN et al, NEJM 2025, PMID 40305708; the approval-indication-establishing trial). Tirzepatide Phase 2 MASH (SYNERGY-NASH, Loomba 2024 PMID 38856224) demonstrated 62% MASH resolution at 15 mg vs 10% placebo and is on a Phase 3 path. Survodutide Phase 2 (Sanyal 2024 PMID 38847460) demonstrated 62% MASH resolution at 6.0 mg vs 14% placebo.
Evidence: Sanyal AJ et al, NEJM 2024 (survodutide Phase 2 MASH) [PMID 38847460]; Loomba R et al, NEJM 2024 (tirzepatide SYNERGY-NASH Phase 2 MASH) [PMID 38856224]; Sanyal AJ et al, Nat Med 2024 (retatrutide Phase 2a MASLD substudy) [PMID 38858523]; Sanyal AJ, Newsome PN et al, NEJM 2025 (ESSENCE semaglutide Phase 3 MASH) [PMID 40305708].
Q9: A patient asks about CagriSema versus tirzepatide or retatrutide — how do I frame the choice?
CagriSema, tirzepatide, and retatrutide all sit at the maximum-effect-size tier of current obesity pharmacotherapy, but they represent three philosophically distinct drug-development strategies:
- CagriSema is a co-formulated combination product (cagrilintide 2.4 mg + semaglutide 2.4 mg in a single weekly injection). REDEFINE-1 demonstrated 22.7% body weight loss at 68 weeks with a 4-arm design that lets clinicians see the component contributions (cagrilintide-alone 11.8%, semaglutide-alone 16.1%, combo 22.7%) — combo effect approximates the arithmetic sum, consistent with additive mechanism integration. Pre-approval-for-marketing-claims; Novo Nordisk regulatory dossier submitted following REDEFINE-1/-2 publications.
- Tirzepatide is an approved single-molecule polyagonist engineered to engage both GLP-1R and GIPR. SURMOUNT-1 (−20.9% at 15 mg / 72 wk) and SURMOUNT-5 head-to-head (−20.2% vs sema 2.4 mg −13.7%) establish the effect-size frontier of the approved class.
- Retatrutide is a pre-approval single-molecule polyagonist engineered to engage GLP-1R, GIPR, and GCGR. TRIUMPH-4 sponsor topline (−28.7% at 12 mg / 68 wk) suggests the highest effect-size tier among currently characterized agents.
The clinical choice is mechanism-class and availability driven: tirzepatide is the approved option with the most direct head-to-head data and the strongest current regulatory standing. Retatrutide is the pre-approval option with the largest effect size in early Phase 3 readout; for patients who reach guideline-criteria threshold today, tirzepatide remains the first-line dual-agonist option, with retatrutide entering the conversation once approved. CagriSema, when approved, will offer the combination-product alternative in the same maximum-effect-size tier, with the operational difference that it is two distinct mechanism classes co-formulated rather than a single engineered molecule.
The patient-counseling beat: present these as three legitimate clinical-translation strategies (combination product vs single-molecule dual agonist vs single-molecule triagonist) at the same effect-size tier. The shared decision-making centers on the patient's specific phenotype, comorbidity profile, insurance coverage, and tolerability priorities — not on a ranking of "best" agent.
Evidence: Garvey WT et al, NEJM 2025 REDEFINE-1 [PMID 40544433]; Davies MJ et al, NEJM 2025 REDEFINE-2 [PMID 40544432]; Jastreboff AM et al, NEJM 2022 SURMOUNT-1 [PMID 35658024]; Aronne LJ et al, NEJM 2025 SURMOUNT-5 [PMID 40353578]; Jastreboff AM et al, NEJM 2023 retatrutide Phase 2 [PMID 37366315]; TRIUMPH-4 sponsor topline December 2025 — peer-reviewed publication PMID pending.
Q10: A patient asks about oral options — oral semaglutide vs orforglipron. What's the difference?
The two oral options in current and near-future use are mechanistically GLP-1 RAs but pharmaceutically distinct platforms:
- oral semaglutide = oral semaglutide + SNAC permeation enhancer. A peptide formulated with sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC) to enhance gastric absorption. Daily dosing; requires fasted administration with up to 4 oz of plain water and ≥30 minutes before food, drink, or other oral medications. SOUL CV outcomes trial (PMID 40162642) established CV benefit in T2D + ASCVD/CKD; approved for T2D.
- Orforglipron = oral non-peptide small-molecule GLP-1 RA. A spiropiperidine-based small molecule that engages GLP-1R via a binding mode distinct from peptide ligands. Room-temperature stability; chemical-synthesis manufacturing (vs solid-phase peptide synthesis); oral bioavailability without permeation enhancer and without food/water timing restrictions. ATTAIN-1 Phase 3 obesity (PMID 40960239) demonstrated −11.2% at 36 mg / 72 wk; NDA submission anticipated end of 2025 obesity / 2026 T2D per Lilly disclosures. Currently pre-approval-for-marketing-claims.
The clinical implications: oral semaglutide is the approved oral option today, with the limitation of strict fasted-administration timing that meaningfully constrains real-world adherence for many patients. Orforglipron, once approved, will be the first oral non-peptide GLP-1 RA — eliminating the food/water timing restriction and the cold-chain supply constraints that the peptide platform requires, with implications for international access, supply chain resilience, and patient adherence.
For the patient who needs oral therapy today: oral semaglutide is the available option, with explicit titration to manage the timing-restriction adherence load. For patients who can wait for approval and prefer oral over subcutaneous: orforglipron will be a meaningful platform option when available.
Evidence: Wharton S et al, NEJM 2025 ATTAIN-1 [PMID 40960239]; Rosenstock J et al, NEJM 2025 ACHIEVE-1 [PMID 40544435]; McGuire DK et al, NEJM 2025 SOUL [PMID 40162642].
Section 8: Evidence Table
| Claim | Source | PMID | Evidence Level |
|---|---|---|---|
| Adaptive thermogenesis 6–8 kcal/kg FFM/day after 10% weight loss | Leibel, Rosenbaum & Hirsch, NEJM 1995 | 7632212 | II (original metabolic-chamber data) |
| Metabolic adaptation persists years after weight loss | Rosenbaum & Leibel, Int J Obes 2010 | 20935667 | II (synthesis review) |
| Adaptive thermogenesis persists ≥1 year post weight loss | Rosenbaum et al, AJCN 2008 | 18842775 | II (matched-trio metabolic ward) |
| Adaptive thermogenesis persists at 6 years (Biggest Loser cohort, −499 ± 207 kcal/day) | Fothergill et al, Obesity 2016 | 27136388 | II (longitudinal cohort) |
| Hormonal adaptation (ghrelin, leptin, PYY, thyroid) persists ≥1 year post weight loss | Sumithran et al, NEJM 2011 | 22029981 | II |
| Lifestyle programs maintain ~3 kg / ~3% body weight at 4–5 years | Anderson et al, AJCN 2001 (meta-analysis 29 studies) | 11684524 | I |
| Look AHEAD: 6.0% loss at median 9.6 yr; no MACE benefit | Wing RR et al, NEJM 2013 | 23796131 | I |
| DPP: 58% T2D incidence reduction at 2.8 yr (lifestyle) | Knowler WC et al, NEJM 2002 | 11832527 | I |
| DPP dose-response: 16% T2D risk reduction per kg loss | Hamman RF et al, Diabetes Care 2006 | 16936160 | I |
| Modern review of weight regain physiology | Hall & Kahan, Med Clin N Am 2018 | 29156185 | III |
| Multi-society advisory: GLP-1 + nutritional/lifestyle support | Mozaffarian et al, Obesity 2025 (ACLM/ASN/OMA/TOS) | 40445127 | III (consensus) / I (underlying) |
| Semaglutide 2.4 mg: −14.9% weight loss (STEP 1) | Wilding et al, NEJM 2021 | 33567185 | I |
| Tirzepatide 15 mg: −20.9% weight loss (SURMOUNT-1 ITT) | Jastreboff et al, NEJM 2022 | 35658024 | I |
| Tirzepatide vs semaglutide head-to-head: −20.2% vs −13.7% (SURMOUNT-5) | Aronne LJ et al, NEJM 2025 | 40353578 | I |
| Liraglutide 3.0 mg: ~−8% weight loss (SCALE) | Pi-Sunyer et al, NEJM 2015 | 26132939 | I |
| Retatrutide Phase 2 obesity: −24.2% at 12 mg / 48 wk | Jastreboff AM, Kaplan LM et al, NEJM 2023 | 37366315 | I (Phase 2 RCT) |
| Retatrutide Phase 2 T2D | Rosenstock J, Frias J et al, Lancet 2023 | 37385280 | I (Phase 2 RCT) |
| Retatrutide Phase 2a MASLD substudy: ~82% MRI-PDFF reduction | Sanyal AJ et al, Nat Med 2024 | 38858523 | I (Phase 2a substudy) |
| Retatrutide TRIUMPH-4 Phase 3 obesity + knee OA: −28.7% at 12 mg / 68 wk | Eli Lilly sponsor topline 2025-12-11 | PMID pending | Sponsor disclosure |
| Survodutide Phase 2 MASH: 62% resolution at 6 mg | Sanyal AJ et al, NEJM 2024 | 38847460 | I (Phase 2 RCT) |
| Tirzepatide Phase 2 MASH (SYNERGY-NASH): 62% resolution at 15 mg | Loomba R et al, NEJM 2024 | 38856224 | I (Phase 2 RCT) |
| Semaglutide Phase 3 MASH (ESSENCE): approval-indication-establishing | Sanyal AJ, Newsome PN et al, NEJM 2025 | 40305708 | I (Phase 3 RCT) |
| CagriSema REDEFINE-1: 22.7% at 68 wk (4-arm) | Garvey WT et al, NEJM 2025 | 40544433 | I (Phase 3 RCT) |
| CagriSema REDEFINE-2: 13.7% vs sema 10.6% in T2D | Davies MJ et al, NEJM 2025 | 40544432 | I (Phase 3 RCT) |
| Cagrilintide-alone REDEFINE-1 arm: 11.8% at 68 wk | Garvey WT et al, NEJM 2025 (4-arm) | 40544433 | I (Phase 3 RCT) |
| Orforglipron ACHIEVE-1 Phase 3 T2D | Rosenstock J et al, NEJM 2025 | 40544435 | I (Phase 3 RCT) |
| Orforglipron ATTAIN-1 Phase 3 obesity: −11.2% at 36 mg / 72 wk | Wharton S et al, NEJM 2025 | 40960239 | I (Phase 3 RCT) |
| Orforglipron ATTAIN-2 Phase 3 obesity + T2D | Horn DB et al, Lancet 2026 | 41275875 | I (Phase 3 RCT) |
| insulin icodec + semaglutide COMBINE 2 (T2D; weight axis: +0.84 kg vs sema −3.70 kg) | Lingvay I et al, Diabetologia 2025 | 39820580 | I (Phase 3 RCT) |
| SELECT — semaglutide CV outcomes (HR 0.80 MACE) | Lincoff AM et al, NEJM 2023 | 37952131 | I (Phase 3 RCT) |
| SOUL — oral sema CV outcomes | McGuire DK et al, NEJM 2025 | 40162642 | I (Phase 3 RCT) |
| STRIDE — sema for PAD | Bonaca MP et al, Lancet 2025 | 40169145 | I (Phase 3 RCT) |
| STEP TEENS — adolescent sema | Weghuber et al, NEJM 2022 | 36322838 | I (Phase 3 RCT) |
| STEP 1 Extension — regain after discontinuation | Wilding et al, DOM 2022 | 35441470 | I |
| Phenotype-guided AOM selection: 15.9% vs 9.0% at 12 mo | Acosta et al, Obesity 2021 | 33759389 | II |
| Genetics of obesity (heritability 40–70%, polygenic + monogenic) | Loos & Yeo, Nat Rev Genet 2022 | 34556834 | III |
| GLP-1 RA cancer SR: "little or no effect" thyroid/pancreatic/breast/kidney (moderate certainty) | Ko A et al, Ann Intern Med 2026 | 41359966 | I (SR+MA, 48 RCTs, n=94,245) |
| GLP-1 RA thyroid cancer signal in French database | Bezin J et al, Diabetes Care 2023 | 36356111 | II (case-control) |
| Rodent C-cell signal foundational paper (class label basis) | Bjerre Knudsen L et al, Endocrinology 2010 | 20203154 | II (mechanism) |
| Pancreatitis class signal: RR 1.44 (95% CI 1.09–1.89) | Wen J et al, Endocrinol Diabetes Metab 2025 | 40988099 | I (SR+MA, 62 RCTs) |
| GLP-1 RA NAION/ION signal | Lakhani M et al, Am J Ophthalmol 2025 | 40383360 | II (pharmacovigilance) |
| Psychiatric protective signal: OR 0.62 (Bezin 2024) | Bezin J et al, EClinicalMedicine 2024 | 39844933 | II (case-time-control) |
| AACE 2025 ABCD algorithm | Nadolsky K, Garvey WT et al, Endocr Pract 2025;31(11):1351-1394 | 40956256 | III (guideline) / I (underlying) |
| EASO 2025 framework | McGowan B, Ciudin A et al, Nat Med 2025;31(10):3229-3232 | 41039115 | III (guideline) |
| Retatrutide discovery + receptor engagement profile | Coskun T, Urva S et al, Cell Metab 2022 | 35985340 | III (mechanism) |
KNOWLEDGE CHECK
Q1: A 48-year-old woman with BMI 34, fasting insulin 22 mU/L, HbA1c 5.9%, triglycerides 188 mg/dL, and MASLD on imaging presents for weight management. Which obesity phenotype BEST describes her presentation, and which mechanism class is the strongest first-line match?
A. Hyperphagic / appetite-driven; single GLP-1 RA
B. Metabolic / insulin-resistant; dual GLP-1/GIP (tirzepatide) — with survodutide or retatrutide as Phase-3-active alternatives where hepatic GCGR engagement is rationale-relevant ✓
C. Hormonal / age-related; GH secretagogue
D. Stubborn-fat / plateau; AOD-9604
Rationale: Elevated fasting insulin, borderline HbA1c, hypertriglyceridemia, and MASLD anchor a metabolic / insulin-resistant phenotype. Tirzepatide (approved dual GLP-1/GIP) is the strongest first-line approved option; survodutide (Phase 3, FDA Breakthrough Therapy MASH) and retatrutide (Phase 3, TRIUMPH-4 topline −28.7%) become available as additional dual / triagonist options as their approval and access mature. Sources: SURMOUNT-1 PMID 35658024; SYNCHRONIZE-1 sponsor topline 2026-04; TRIUMPH-4 sponsor topline 2025-12-11.
Q2: Which of the following BEST explains why metabolic adaptation makes sustained weight loss difficult without pharmacologic support?
A. Patients lose motivation after initial weight loss
B. Exercise capacity decreases with lower body weight
C. Reduced resting metabolic rate (Leibel ~6–8 kcal/kg FFM/day at 10% loss; Fothergill ~500 kcal/day at 6 years), increased ghrelin, decreased leptin/PYY/thyroid hormones, persisting at multi-year timescales — a coordinated hormonal headwind that is not extinguishable through behavior alone ✓
D. Genetic predisposition prevents weight loss beyond a certain point
Rationale: Metabolic adaptation involves measurable hormonal and metabolic changes that persist at >1 year (Rosenbaum 2008 PMID 18842775; Sumithran 2011 PMID 22029981) and at 6 years (Fothergill 2016 PMID 27136388). This creates a physiological drive toward weight regain that is independent of patient motivation, and is the principal reason pharmacotherapy is the rate-limiting input for sustained loss in most patients.
Q3: A patient's lab results show: IGF-1 of 95 ng/mL (low-normal), free testosterone 8.2 pg/mL (low), TSH 3.8 mIU/L, with gradual 30-lb weight gain over 10 years. Which approach is MOST aligned with this phenotype?
A. Semaglutide 2.4 mg weekly for appetite suppression
B. AOD-9604 for localized fat mobilization
C. CJC-1295/Ipamorelin + hormonal optimization (TRT consideration), with GLP-1 RA layered as needed for the weight-management indication and explicit M5.6 lean-mass preservation protocol ✓
D. MOTS-c for mitochondrial metabolic flexibility
Rationale: Low IGF-1, low free testosterone, and gradual age-related weight gain indicate hormonal / age-related obesity (Phenotype 3). GH secretagogues address the GH/IGF-1 axis decline, and TRT evaluation is warranted for the low testosterone. GLP-1 RA is layered where the weight-management indication is present, with explicit lean-mass-preservation discipline because the GLP-1 axis on its own does not preferentially preserve muscle.
Q4: Which of the following best characterizes the current 2026 evidence state for GLP-1 RA cancer surveillance?
A. The class shows a clear increased thyroid cancer signal that warrants routine calcitonin screening
B. The 2026 SR+MA (Ko et al, 48 RCTs, n=94,245, PMID 41359966) reports "little or no effect" on thyroid / pancreatic / breast / kidney cancer with moderate certainty; the MTC/MEN2 absolute contraindication remains; the pancreatitis class signal (Wen 2025 RR 1.44) and the semaglutide-class NAION signal (Lakhani 2025) are distinct active-surveillance areas ✓
C. The 2024 psychiatric warning has been confirmed across multiple databases
D. All cancer concerns have been resolved by post-marketing surveillance
Rationale: The class-level safety state in 2026 is granular and requires class-differentiation framing. Ko 2026 reports moderate-certainty "little or no effect" across the major cancers; the MTC/MEN2 absolute contraindication remains anchored in the rodent C-cell signal (Bjerre Knudsen 2010 PMID 20203154); pancreatitis class signal is real (Wen 2025 RR 1.44, PMID 40988099) with discontinuation if acute pancreatitis develops; NAION class-differentiation favors semaglutide-class signal documented vs tirzepatide-class signal absent at threshold (with exposure-window asymmetry caveat); psychiatric concern reframed by Bezin 2024 (PMID 39844933) protective OR 0.62. The pattern: each safety signal requires its own evidence-state characterization.
CLINICAL APPLICATION
Scenario: You are evaluating a new weight loss patient. Create a 4-step phenotyping and mechanism-class-selection assessment:
- Review intake labs (fasting insulin, glucose, HbA1c, lipid panel, IGF-1, free testosterone, TSH/free T3, leptin) and imaging (waist circumference, body composition, MASLD screening where indicated)
- Classify primary phenotype (1–4) and any secondary overlay based on lab pattern + clinical presentation + family history + hunger/satiety self-report
- Map phenotype to mechanism class (single GLP-1 RA / dual GLP-1+GIP / dual GLP-1+glucagon / triagonist / amylin axis / combo product / GH-axis adjunct / lipolysis adjunct) per Section 2 taxonomy
- Identify the specific approved first-line agent within the chosen mechanism class, with Phase-3-active alternatives noted for tracking
Document your reasoning for a hypothetical patient with: BMI 38, fasting insulin 28 mU/L, HbA1c 6.2%, triglycerides 220 mg/dL, normal IGF-1, mild MASLD on ultrasound, history of three failed diet attempts.
Related Clinical Protocols
For deeper clinical implementation, see the companion protocol files:
- Master Protocol Index — navigation hub for all 14 Module 5 clinical protocols
- Phenotype-Guided Decision Tree Protocol — patient-phenotype routing logic for compound selection
- Pre-Treatment Metabolic Preparation Stack Protocol — body-priming peptides (BPC-157, SS-31, KPV, TB-500, Selank, DSIP, NAD+) BEFORE GLP-1 initiation
Resources & Downloads
Lesson package — clinician protocols, patient handouts, the knowledge check, and the full zip bundle.
Lesson Package Index
Baseline Labs Checklist
Phenotype to Peptide Decision Matrix
Compounding Pharmacy Quality Audit Checklist
Reconstitution One Pager
Hormone Optimization Peptide Reference Card
Informed Consent Template Compounded Peptide Therapy
Patient Handout What to Expect on Semaglutide
Patient Handout Self Injection Technique
Trial Portfolio Summary Cards
5 Safety Fronts Deep Dive
Knowledge Check
Treatment Initiation Protocol
DOCX
Final Narration Script for Clinical Review
Final Narration Script for Clinical Review
ZIP
Lesson Package